

Since graduating in 1983 I have been in private practice and Neural Integration is the culmination of treating over twelve thousand patients, and continuous research over this period. The methods employed are an adaptation of numerous, well established, proven and relatively gentle chiropractic techniques, most of which are not in common use today. Therefore treatment protocols do not resemble chiropractic as most people have come to recognise it.
I am particularly grateful to my mentor and friend, the late Dr Carl Ferrari from New York for his teaching and continued support in my early years. The primary aim of Neural Integration being to specifically address the cause/s of chronic pain and other neural related symptoms, and to bring about regenerative self healing, thus promoting health restoration naturally, logically, and on purpose.
As shown throughout, there exists an extensive body of documented literature regarding the deleterious effects of vaccines, with regard to the effect that heavy metal toxins have on the human brain and nervous system. Especially with regard to developing and later stage neurocognitive ability. But while vaccines contain toxic materials that are injected directly into the body, “toxic overload’ is also caused by environmental hazards. These include lead and mercury exposure, air pollution, chemtrails, and organic compounds, given that all have the potential to damage brain function, yet remain understudied.
In other words predisposing factors begin with maternal health, including ongoing healthy conditions or lifestyle factors during pregnancy, any harmful maternal medications taken during pregnancy, and as just mentioned, maternal environmental pollutant exposure. Together with the advantage of immune supporting breast feeding, immune supporting diets, and specific suppliants. With regard to genetic predisposing factors, if according to science, genetic changes can occur over millions of years, then given that the current epidemic of autism, dementia, mental illness and cognitive decline has occurred within one or two generations, how can this be genetics when toxic reactivity makes far more sense, as will hopefully become clear.
Contents
Introduction (Home page)
Part 1: About Neural Integration - Unlocking the Body’s Innate Potential for Self Healing
Part 1: PDF Download
Part 2: Incompetence or Intent?
Part 2: PDF Download
Part 3: Who in their right mind would trust WHO? & Government Collusion
Part 3: PDF Download
Part 4: Agenda 2030, Vaccine Related Health Damage and 5G Implications
Part 4: PDF Download
Part 5: Studies Showing The Unvaccinated are Healthier & Fake Science
Part 5: PDF Download
Part 6: The Hidden Hands of the Puppeteers
Part 6: PDF Download
Part 7: Trump, Russia & the Kings from the East
Part 7.1: PDF Download
Part 7.2: PDF Download
Part One: Discusses Neural Integration logic and method: click ‘Part 1 ‘About Neural Integration’ above to open. Parts Two to Seven discuss the reasons behind the widespread health damage and excess deaths caused by the Covid vaccines, and the ongoing epidemic of medically induced mental & physical health issues. To those naive enough to believe that all vaccines are “safe and effective” I would strongly suggest you read the data showing the millions of excess deaths and vaccine related damage, after which any critical thinking person should be left in very little doubt.
I have been treating vaccine damaged babies, children and adults throughout my 40 year career as a primary health care professional and can state unequivocally like many other physicians and other health care professionals, that I also am in no doubt that vaccines can and do cause serious mental and physical health problems. If vaccines really cause no lasting harm then why have so many billions been paid to ruined families in compensation?

Adverse prescription drug reactions cause up to 20% of emergency hospital admissions
According to AI, studies indicate that adverse prescription drug reactions are a major driver of hospital emergency admissions. In fact updated research show that up to 16.5% to 20% are caused by complications from commonly prescribed medicines. In addition to A & E admissions, actual prescription medication and administration errors are estimated to be annually around 237 million medication errors in England alone.
But this has been going on for decades, in fact in February 2018 a Sky News headline warned: “NHS medicine errors may have contributed to 22,000 deaths a year.” In response the Health Secretary Jeremy Hunt at that time told Sky News: "Medication errors is not higher in the NHS than in it is in EU countries or the United States.” NHS Ref: https://pmc.ncbi.nlm.nih.gov/articles PMC2093926/
Nothing in life is risk free, and that includes vaccines, but without any objective proof, medical doctors are taught that children are more at risk from not being vaccinated. As if somehow God forgot to provide all babies with healthy immune systems. In reality it is the mother that transfers her antibodies to the baby during pregnancy through the placenta and through breast milk, particularly colostrum, thus providing protection against various infections. Rather that blindly accept that all vaccines are safe, parents should push back against the same fake scaremongering that was used to push the Covid vaccines.
Not least because like the Covid vaccine, the average medical doctor does not have a clue what is inside most vaccines, or has ever done any objective research regarding the plethora of well documented harmful side effects. If you doubt this then before allowing them to inject your baby, ask the doctor to name at least five of the ingredients, also what the effects of those ingredients are, and what, if any are the proven immune system benefits? - without googling the information. You’ll probably experience a long awkward silence, but no answers; shocking but true. In America, and similarly in the UK children receive multiple vaccinations against diseases by the time they start school. These include vaccines for measles, mumps, rubella, varicella (chickenpox), hepatitis A, hepatitis B, diphtheria, tetanus, pertussis (whooping cough), Haemophilus influenzae type b (Hib), polio, influenza (flu), rotavirus, and pneumococcal disease, dengue fever and now COVID-19.
Now ask yourself why were all the packaging information inserts for COVID-19 vaccines left suspiciously blank, thus deliberately leaving out vital information concerning the ingredients and the related harmful side effects they already knew of as shown below. Blank sheets that should start ringing warning bells in most thinking people, but obviously not the medical doctors. They were more than happy to comply, i.e. repeatedly injecting vulnerable infants, the elderly, and anyone else naive enough to believe the spin. Some were even filmed dancing around the corridors, as if everything was just fine and dandy, but as a result of their criminal negligence, millions have since died, and many more left with life changing side effects due to the ongoing DNA corruption. A fact that had previously and repeatedly been denied, but since admitted.

January 5th 2026
In December President Trump ordered changes to the immunisation schedule and directed Kennedy and the CDC to review vaccine recommendations. Vaccine hesitancy and concerns regarding their safety and long term adverse side effects has been growing steadily for decades. Experts are noticing an ongoing trend regarding reduced public confidence in mandatory vaccine schedules. Which also raises the question: if, as we have been led to believe, all infant and childhood vaccines have been ‘proven’ to be necessary, safe and effective, then why are the revised US childhood immunisation guidelines being so radically reduced? The new recommendations were made in response to an executive order signed by President Trump in December, the US health department said. That order instructed US health officials to compare the country to "peer developed countries" and make recommendations.
"Many Americans, especially the "MAHA Moms," have been praying for these COMMON SENSE reforms for many years," Trump said in a statement online referring to the Make America Healthy Again slogan. The loss of trust in the COVID vaccines coincided with less adherence to the full CDC childhood vaccine schedule, which has resulted in lower immunisation rates of well-established vaccines, such as those for measles, rubella, pertussis, and polio. The new schedule will also no longer universally recommend immunisation against meningitis, hepatitis A and B, (discussed below) respiratory syncytial virus (RSV), rotavirus, COVID-19, and influenza.
In 2022, Denmark became the first peer nation to remove its universal recommendation of the COVID-19 vaccine for children, with the director of its public health authority recognising that there was little benefit in giving this vaccine to children. Since then, all other peer nations have followed. At their September 2025 meeting, the ACIP voted that shared clinical decision-making should be applied to the COVID-19 vaccine for U.S. children and adolescents. Since the Covid vaccine rollout we have seen increasing reports and studies all of which indicate a rise in heart disease risk factors and conditions, including heart attacks and heart failure, in children and adolescents. See Parts 2 & 5
“The goal of this administration is to basically make vaccines optional,” said Paul Offit, an infectious diseases physician at Children’s Hospital of Philadelphia and a former member of the advisory committee on vaccines for the US Food and Drug Administration (FDA). In response the Institute of Medicine stated in a report that "vaccines-like all drugs or medical interventions, are neither 100 percent risk-free nor 100 percent effective.”

Dr. Toby Rogers is a political economist and researcher, and the above quote is from Dr Rogers during a fiery congressional hearing on September 9-10, 2025, titled "How the Corruption of Science Has Impacted Public Perception and Policies Regarding Vaccines.” The study, led by researchers at Henry Ford Health, examined medical records of roughly 18,500 children born between 2000 and 2016, comparing chronic illnesses in vaccinated versus unvaccinated groups.
Dr. Rogers argued that COVID-19 vaccines carried "the worst side effects" and claimed that the autism/chronic disease epidemic is linked to toxicant exposure, advocating for a halt to certain vaccine schedules. Chaired by Senator Ron Johnson it soon turned into a heated debate over the unpublished 2020 study.
“The study found that exposure to vaccination was independently associated with an overall 2.5-fold increase in the likelihood of developing a chronic health condition, when compared to children unexposed to vaccination.”
This association was primarily driven by asthma, atopic disease, eczema, autoimmune disease and neurodevelopmental disorders. (ranging from learning difficulties to severe autism) This suggests that in certain children, exposure to vaccination may increase the likelihood of developing a chronic health condition, particularly for one of these conditions. NB Similar studies are included in Part 5 together with my own nationally published study of children with learning difficulties and other related problems. All children were assessed pre and post treatment. The neurological improvements were undeniable as reported by the Daily telegraph, the National children’s bureau, and others.
The following is taken from the above cited congressional hearing that begins with Senator Johnson, “Our second hearing allowed witnesses who have been impacted by vaccine injuries and fatal infectious diseases to tell their stories. The news media is all too willing to highlight a new outbreak of an infectious disease, but is loath to broadcast what they generally describe as "rare and mild" vaccine injuries. As a result, the vaccine injured had been ignored and abandoned… They certainly don't want the public to know the root cause if it's one of their products and they're willing to go to great lengths by spending billions of dollars on advertising and lobbyists to keep the public from even asking the question, much less finding the answer. The purpose of these hearings is to force the acknowledgment of reality.”
Senator Johnson continues, “It’s been interesting to see the media's reaction to our previous hearings, except for a few highly biased attack pieces. The legacy media has largely ignored what I consider to be highly informative hearings. Perhaps they're taking advice from Senator Blumenthal who hours before our last hearing, Voices of the Vaccine Injured, held a press conference and was reported to have stated”…."I hope nothing comes of this hearing. I hope people don't pay attention because it isn't deserving of credibility and attention." However, during that hearing Senator Blumenthal stated, "I'm heartbroken to hear these stories. It makes me want to do something". So maybe hearing true incredible stories of accident injuries actually did deserve attention. I certainly believe today's testimony deserves attention and hope it will prompt us to do something to restore credibility and integrity to science and our federal health agencies.”

Recent reporting by the Daily Mail has reignited discussion around whether a complication linked to COVID-19 vaccines could help explain a growing number of unexplained illnesses reported by some individuals. The article draws attention to patients who say they developed persistent symptoms shortly after vaccination, prompting renewed scientific interest in how the immune system may respond differently in a very small subset of people. According to the report, researchers are exploring the possibility that in rare cases, the immune response triggered by COVID-19 vaccines may fail to properly resolve, potentially leading to prolonged inflammation or immune dysregulation.
Individuals featured in the article describe symptoms such as extreme fatigue, brain fog, dizziness, heart palpitations, and neurological issues that they say began days or weeks after receiving a vaccine dose. One patient reportedly said they felt as though their “body was constantly stuck in fight-or-flight mode.” The article cites scientists who suggest these symptoms may resemble those seen in long COVID, raising the question of whether a similar mechanism could be involved.
One researcher quoted in the piece stated that the condition appears to be “immune-mediated,” meaning the immune system itself may be driving ongoing symptoms rather than an active infection. Another expert noted that while such reactions appear to be rare, “even a small percentage can translate into a significant number of people when billions of doses are administered.” Medical authorities have previously acknowledged that rare adverse events can occur following vaccination. Conditions such as myocarditis, particularly in younger males, and certain clotting disorders associated with earlier adenovirus-based vaccines were identified through post-marketing surveillance.
One clinician emphasised that “these cases require careful study and should not be dismissed, but they must also not be overstated without robust evidence.” Large-scale, peer-reviewed studies are still needed to determine whether a distinct post-vaccination syndrome exists and, if so, how frequently it occurs. Researchers involved in ongoing studies reportedly acknowledge that medicine has not yet fully mapped the long-term immune effects of COVID-19 infection or vaccination, particularly in people with underlying autoimmune tendencies. As one scientist quoted in the article explained, “The immune system is extraordinarily complex, and in rare cases, it may react in ways we don’t yet fully understand.”
https://endtimeheadlines.org/2025/12/new-study-claims-reveals-rare-complication-linked-to-covid-vaccines-that-causes-life-threatening-immune-disorder/
When Fools are Given Credibility They Become a Liability:
Andrew Bridgen, is an self-made, ex-military man and former Member of Parliament who in spite of coming from a working-class background, built a very successful career in business. After building a 30 million pound business employing 300 people he decided he wanted to give something back and so went on to serve as the Member of Parliament for North West Leicestershire for 14 years, until 30 May 2024. During those 14 years he elevated the non-metropolitan district of North West Leicestershire from being the poorest to the richest. But as discussed in Part Two, after a tumultuous journey as a political rebel, whistle-blower and vocal critic of COVID-19 vaccines, Mr. Bridgen had the Conservative whip removed in January 2023, and was expelled from the party on April 12, 2023.
Having a background in biological sciences, Bridgen was troubled by the silencing of scientists who had expressed concerns about the safety and efficacy of the new untested vaccines. Andrew Bridgen: “I knew that there would be a huge establishment backlash the moment I spoke out against the vaccination of small children. I tried to recruit colleagues to help me. I went to my old Brexiteer friends and the response was shocking. Some of them said that they had also suffered side effects themselves and believed there was something wrong with the vaccines. Some of them told me that they’d had relatives who were severely injured. But to a man and a woman, they said they weren’t going to speak out about it.”
In an historical tightly packed and extraordinary vocally loud public gallery, threatened with removal, and with hundreds more outside who could not get in, in direct contrast to an almost empty Chamber of MP’s, on April 18, 2024, MP Andrew Bridgen opened a House of Commons debate on "Covid-19: Response and Excess Deaths.” https://hansard.parliament.uk/commons/2024-04-18/debates/9F01F787-D758-43D4-B8D14FA357EB3EED/Covid-19ResponseAndExcessDeaths
During which Mr. Bridgen referred to a cardiologist who had told him the vaccine rollout was, to quote: "the biggest crime against humanity since the Holocaust.” Based on his own research, Bridgen himself also claimed the Covid-19 vaccines had contributed significantly to excess mortality in 2022 and 2023. He described the excess deaths as a major scandal and urged the government to stop their use, calling them "unsafe, ineffective, and unnecessary.” He also called for the government to release data and for the Covid-19 Inquiry to expedite its investigation into vaccines.

Andrew Bridgen: “We are witnesses to the greatest medical scandal in this country in living memory, and possibly ever: the excess deaths in 2022 and 2023. Its causes are complex, but the novel and untested medical treatment described as a covid vaccine is a large part of the problem. I have been called an anti-vaxxer, as if I have rejected those vaccines based on some ideology. I want to state clearly and unequivocally that I have not: in fact, I am double vaccinated and vaccine-harmed. Intelligent people must be able to tell when people are neither pro-vax nor anti-vax, but are against a product that does not work and causes enormous harm to a percentage of the people who take it. I am proud to be one of the few Members of Parliament with a science degree. It is a great shame that there are not more Members with a science background in this place; maybe if there were, there would be less reliance on Whips Office briefings and more independent research, and perhaps less group-think. I say to the House in all seriousness that this debate and others like it are going to be pored over by future generations, who will be genuinely agog that the evidence has been ignored for so long, that genuine concerns were disregarded, and that those raising them were gaslit, smeared and vilified.”
Fast forward to the conclusion: “The evidence is clear: these vaccines have caused deaths. Despite that, they have been described as “safe and effective”. However, for a proportion of people who took them, the vaccines have caused serious harm and death, and they will have raised the risk of cancer for many more. Nor are they effective. The vaccine does not prevent infection or transmission, and when the data is looked at objectively, it shows that the vaccine does not prevent serious illness or death. Those are hard truths to face, but we must face them if we want to learn the lessons of the last few years. At some point we will have to face up to all the evidence that is building. It was fairly convincing 18 months ago when I first spoke out, but it is unequivocal now."
It is also noteworthy that in January 2022, Mr. Bridgen was offered a bribe in exchange for his silence. “I was offered anything I wanted. All I had to do was tell them what I wanted and they’d sort it for me,” he said. So he requested the Prime Minister’s resignation letter. “They told me I couldn’t have that so I said I didn’t want anything else. And we were on a pretty much a collision course from that day onwards.”
He spoke about the backlash surrounding his comment regarding the Covid vaccines being the biggest crime against humanity since the Holocaust; and, how the vulnerable elderly in care homes being killed with midazolam and morphine. In fact Mr. Bridgen believes that 35,000 vulnerable, elderly people in hospitals were euthanised with midazolam and morphine and then recorded as covid deaths. However Mr. Bridgen also sees no hope in corporate media exposing the lies. He also points out, that a guiding principle in medical education is that "half of what doctors are taught in medical school will be disproven or out of date in ten years" a fact widely accepted.
Like a growing number of people in the UK, Mr. Bridgen also accuses the establishment of suppressing evidence regarding rape gang and child-trafficking cases, and how they intimidate whistleblowers, use political blackmail, and that the system will protect itself at all costs. In fact Mr. Bridgen paints a very sobering picture of the current political landscape, exposing the gulf between public perception and behind-the-scenes reality. He argues that the freedoms we take for granted are in jeopardy, outlining the potential consequences if more action isn’t taken. As Mr. Bridgen points out, those people in positions of power have betrayed humanity for personal gain, and it will be impossible to reverse this betrayal. The globalists have a plan for humanity that is “dark,” but people are starting to wake up to this plan.
He continues: “It doesn’t matter how many times the people vote and make their views heard. It doesn’t matter which party is in government because our politicians at the top are not serving the people. They’re enthralled to their masters, and that is the World Economic Forum, agenda 2030 and everything that’s involved in that, which is the breaking down of all, it’s the end of sovereign nations, mass migration. That’s where it’s all going. And everything else around our politics is a pantomime to amuse the people. The politicians are only temporary holders of power and true power resides with the people. But the freedoms we take for granted are in jeopardy, outlining the potential consequences if more action isn’t taken.”
Mr. Bridgen also speaks of his early attempts to expose the Post Office Horizon scandal, years before it made headlines; about the unseen forces controlling politicians and silencing dissenters; personal experiences of political suppression and the cost of speaking truth to power; the looming threats to global freedoms and civil liberties and issues an urgent call to action for humanity to reclaim its autonomy. Because as history shows, anyone who is willing to give up their freedom for security, ends up with neither freedom or security. In other words, what the government is trying to convince people is that our freedom is a privilege, in spite of the fact it is a fundamental, inalienable human right, and it belongs to everyone equally without needing to be earned.
But what we are seeing here is mirroring Chinese totalitarian control. Where privileges are removed if the government considers a persons behaviour ‘unsuitable’ to its agenda. When Tony Blair, who is a very evil man, led New Labour to power in 1997 the first piece of legislation he put through the House of Commons after years in opposition, was to remove the death penalty for Treason, and looking back the reason is now becoming obvious. Because, not only Blair, but every government since has committed treason against the British people. Why else after 17 years in opposition was their first priority to remove this act? Because they knew what that had planned. The evidence of which speaks for itself. The Remedy: bring back hanging for murder and treason against the people.

Retired Dr John Campbell has over 3 million YouTube subscribers and his channel has received over 750 million views, especially regarding the safety concerns over the COVID-19 vaccine jabs. On the 15 November 2025 The Daily Telegraph published an article entitled “Government withholding data that may link Covid jab to excess deaths.” In response the UK Health Security Agency argued that “releasing these figures would lead to ‘distress’ of bereaved relatives if connection were discovered.”
In his video posted on 9th December 2025, Dr Campbell comments on the above article and his suspicion’s why the British government is still withholding vital data on vaccine related deaths. In it he confirms that he has received many, many hundreds of emails from viewers, saying that their loved ones, relatives, mothers, fathers, sons and daughters got sick after receiving the COVID vaccines, and that many of them are no longer with us. But what other reason can there be for the British public health watchdog refusing to publish data, other than the British British government is running scared? See Part 2.
Given that the NHS for decades cynically buried all the evidence regarding poor care in a “cover-up culture” that lead to countless avoidable deaths, and families being denied the truth about their loved ones, the NHS ombudsman has warned. “Ministers, NHS leaders and hospital boards are doing too little to end the health service’s deeply ingrained “cover-up culture” and victimisation of staff who turn whistleblower.”
For example the Infected Blood Inquiry, which investigated the contamination of blood and blood products with HIV and hepatitis viruses in the UK between the 1970s and early 1990s considered the biggest treatment disaster in NHS history, was a result of failures by British government, the civil service, and NHS, being involved a decades-long cover-up to conceal the truth. So why would deaths and severe injuries caused by the COVID-19 vaccine jabs be any different? Dr Campbell asks, “If we're not prepared to learn lessons about why people are dying, then what sort of society are we? Is the reason why they are not telling you how your mum died is because it might upset you?” What other can there be, other than trying to save their own skins?
Dr Campbell continues, “it shows their patronising mindset which was also characterised by the pandemic response, i.e. do what we say say, don't ask questions….they are desperate to avoid having to answer that question in public. We know the Government has the data, as do the Quangos and the Pharmaceutical companies, but you and me haven't. Why?” …”Are we just expected to accept what they say, and be thankful to the government for protecting us from mental distress?” End.
The following is taken directly from the aforementioned Telegraph article:
The public health watchdog has been accused of a “cover-up” after refusing to publish data that could link the Covid vaccine to excess deaths. The UK Health Security Agency (UKHSA) argued that releasing the data would lead to the “distress” of bereaved relatives if a link were to be discovered. Public health officials also argued that publishing the data risked damaging the well-being and mental health of the families and friends of people who died.
Last year, a cross-party group expressed alarm about “growing public and professional concerns” over the UK’s rates of excess deaths since 2020. In a letter to UKHSA and Department for Health, the MPs and peers said that potentially critical data, which map the date of people’s Covid vaccine doses to the date of their deaths had been released to pharmaceutical companies but not put into the public domain. They argued that the data should be released “on the same anonymised basis that it was shared with the pharmaceutical groups, and there seems to be no credible reason why that should not be done immediately.”
UsForThem, a UK-based parent-led campaign group that emerged during the COVID-19 pandemic requested that UKHSA release the data under freedom of information laws. But the agency refused, making a number of different arguments including that publishing the data “could lead to misinformation” that would “have an adverse impact on vaccine uptake” in the public. UKHSA also claimed there would be a risk of individuals being identified, despite the request being made for an anonymised dataset. After a two-year battle, the Information Commissioner ruled in the UKHSA’s favour, backing its refusal to publish the data. Campaigners want data that could show if there is a link between mass vaccination against Covid and the UK’s rate of excess deaths to be released. (See charts below)
Reform UK has committed to a public inquiry into excess deaths and alleged Covid vaccine harms. Richard Tice, the party’s deputy leader, said: “We knew there was concern about excess deaths, which is why we called for an inquiry. Instead, the unelected quango UKHSA is involved in a scandalous cover-up of how and why people are dying. This is totally unacceptable, and the Health Secretary must overrule them. If we are not prepared to learn lessons about why people are dying, what sort of society are we?”
Ben Kingsley, the legal director of UsForThem, said the way the UKHSA had handled the case “reveals a desperation that this data should not, in any form, see the light of day.” He added: “It is perverse for UKHSA to argue that this data should not be released because the public could feel distressed or angry if patterns or correlations were to be identified. “You have to ask yourself why it is that the public are considered incapable of handling this data. It reveals a patronising mindset, which also characterised the pandemic response ‘do what we say, don’t ask any questions, we know what is best for you’.”
Mr Kingsley said the Government’s approach appeared similar to the response to the infected blood scandal, in which thousands of people contracted HIV and hepatitis C from contaminated blood products. “The infected blood inquiry published its report while this case was under way,” he said. “We learnt that for years and years the government didn’t think the public could handle the truth, so they kept it from us. “Now we are seeing very similar behaviour from the UKHSA, we don’t know if the data would reveal any evidence of correlation, let alone causation, but we can see they are desperate to avoid having to answer that question in public.”
A UKHSA spokesman said: “Protecting patient confidentiality is of critical importance. Releasing this data presented a real possibility that it could be used to identify individuals, which could result in significant distress. “UKHSA provided a carefully anonymised version of the dataset that removed the risk of identification. We welcome the decision of the tribunal to dismiss the appeal.” - Camilla Turner, Sunday Telegraph Political Editor.
On the 1st Dec 2025 the U.S. Senate’s Permanent Subcommittee on Investigations held a crucial hearing titled "The Corruption of Science and Federal Health Agencies: How Health Officials Downplayed and Hid Myocarditis and Other Adverse Events Associated with the COVID-19 Vaccines." Top medical experts and legal voices testified, including Dr. Peter McCullough, Dr. Jordan Vaughn, Dr. James Thorp, Dr. Joel Wallskog, Attorney Aaron Siri and Hawaii Governor Josh Green. Dr. McCullough presented findings from a large autopsy series, stating that in 73.9% of examined post-vaccine deaths, mRNA COVID vaccines were considered the likely cause, a claim that has sparked intense debate in the medical community.
Given there is a good deal of evidence showing the coronavirus was genetically engineered in Wuhan, China, does this explain why, as shown below during the 2019 COVID-19 pandemic, the influenza virus was non-existent? Given that Big Pharma receives billions every winter from the Flu jabs, might this also suggest the many strains of yearly influenza virus’s are also being genetically engineered?

According to AI: The current 2025/2026 flu season, the UK is seeing a higher number of people vaccinated so far compared to the same point last year. But does this make sense when one considers the UK Flu jab uptake substantially increased prior to the outbreak? Because if the Flu vaccines, like the Covid vaccines really are “safe and effective” then why is the UK suffering from a so-called Flu-nami explosion, with record number of Britons being hospitalised with flu? Prompting the NHS to warn the UK is set for 'worst year with hospital admissions rates rising to almost four times the number seen at the same time last year, and ten times that of the same period in 2023.
As discussed in Part 2, there are studies, such as the one cited below from early 2025, that not only show negative vaccine effectiveness, but in fact demonstrate higher flu rates in those vaccinated. The study concludes, “Among 53402 employees, 43857 (82.1%) that had received the influenza vaccine by the end of the study the cumulative incidence of influenza increased more rapidly among the vaccinated than the unvaccinated.”

With this in mind, the following is taken from John Leake & Medical doctor Peter A. McCullough’s excellent book, ‘Vaccines: Mythology, Ideology, and Reality’ Specifically extracts from Chapter 13 entitled ‘Influenza di Pharma’.

The only enduring lessons learned from the 1976 Swine Flu fiasco were pernicious ones acquired by the pharmaceutical industry. The timeline of the affair raises the suspicion that drug companies opportunistically used sympathetic CDC insiders to exaggerate the purported threat of pandemic swine flu erupting in the fall of 1976. Likewise, the drug companies apparently persuaded the same government insiders to recommend that Congress grant liability protection to vaccine manufacturers. The result yielded a bonanza for Big Pharma while leaving hundreds of Americans suffering from Guillain-Barré syndrome and taxpayers holding the bag.
On June 11, 2009, the World Health Organization declared a new A (HINI) influenza swine flu pandemic based mostly on questionable data from Mexico. The claim that the virus was novel was based entirely on the claim of molecular biologists that the HIN1 variant displayed signs of reassortment, i.e. that two different viruses had apparently infected a host at the same time and re-assorted into a new highly pathogenic killer virus.
But no evidence of this theory was forthcoming in the real world. On the contrary, that virtually no one over the age of sixty developed severe disease indicated that older people had already been exposed to a similar virus decades earlier. Those who were infected developed mild symptoms and the mortality rate was much lower than that of the 2009 seasonal flu. Nevertheless, the WHO pandemic declaration triggered governments all over the world to pre-purchase billions of new swine flu vaccines and antiviral medications that proved to be useless.
Once again, so-called "pandemic" proved to be a colossal windfall for Big Pharma while leaving taxpayers holding the bag. The 2009 Swine Flu had proven profitable, but it was doubtful that the influenza industry could keep the gravy train rolling without the emergence of a serious dis-ease. And so, because nature still hadn't yielded a virulent new strain, the virologists Yoshihiro Kawaoka and Ron Fouchier decided to create one.
Far more terrifying than the swine flu virus of the phony 2009 pandemic was the avian influenza, especially H5N1, which has been shown to have a high mortality rate (60 percent of reported human cases in which the patient sought urgent medical care) but has never achieved human-to-human transmission. By 2011, both Kawaoka (University of Wisconsin-Madison and Fouchier (Erasmus Medical Center, Netherlands) independently conducted experiments to assess whether HSN1 could become transmissible between mammals. Ferrets, whose respiratory tract physiology closely resembles the human, were used as the animal model.
Fouchier's team began with an H5N1 strain isolated in Indonesia and introduced specific mutations: two in the hemagglutinin (HA) protein to change receptor binding from avian-type to human-type, and one in the PB2 polymerase gene to enhance replication in mammalian cells. They then serially passaged the virus through ferrets, and after ten passages, observed airborne transmission between ferrets in adjacent cages. Five mutations in total were identified as critical for this transmissibility. Kawaoka's group generated a reassortment virus combining the HA gene from HSN1 with seven segments from the 2009 HIN1 pandemic strain, which already had efficient human transmissibility. They engineered four mutations in the HA protein, enabling respiratory droplet transmission in ferrets.
Both manuscripts were submitted in 2011 and sparked widespread alarm in the scientific community. The U.S. National Science Advisory Board for Biosecurity (NSABB) recommended redacting key methodological details due to bioterrorism and biosafety concerns. This led to a temporary publication delay. After further debate, including international input and the development of new biosafety guidelines, both papers were published, Kawaoka's in May 2012 and Fouchier's in June. The episode ignited an ongoing global debate over the ethics and safety of creating highly pathogenic agents that could, accidentally or deliberately, be released from a lab.
Fouchier and Kawaoka claimed their research enables mankind to stay ahead of the natural evolution of influenza viruses to prepare for their eventual emergence. Equipped with these pathogens, researchers could, they claimed, develop vaccines and antiviral medications to counter them if viruses like them should ever strike. The trouble with this dubious reasoning is that such dangerous pathogens are far more likely to ‘escape’ from a lab than to evolve naturally a purely theoretical prospect that may never happen in millions of years. But in 2020, humanity would learn the hard way how dangerous it is to engineer pathogenic and highly transmissible agents in a lab.
The totality of evidence strongly suggests that, as the FDA virologist Dr. J. Anthony Morris stated in the summer of 1976 the Flu vaccines don't work. The influenza virus antigenically drifts and shifts, enabling it to evade antibody coverage. The very failure of flu vaccines to provide reliable and lasting protection is what enables their manufacturers to sell new ones every year. Any other product that had to be replaced every September and probably still didn't work would quickly lose all customers. It's a testament to the mystical hold that vaccines have on the human mind that many who have received the annual flu shots still get Flu but then get the next year's shot.
In addition to their lack of efficacy, influenza vaccines still cause many injuries every year. Indeed, most payouts from the National Vaccine Injury Compensation Program, established by the National Childhood Vaccine Injury Act of 1986 are for severe adverse reactions to influenza vaccines.”End - NB Underlining mine

by Angeline Tan | Remnant Columnist - December 22nd, 2025
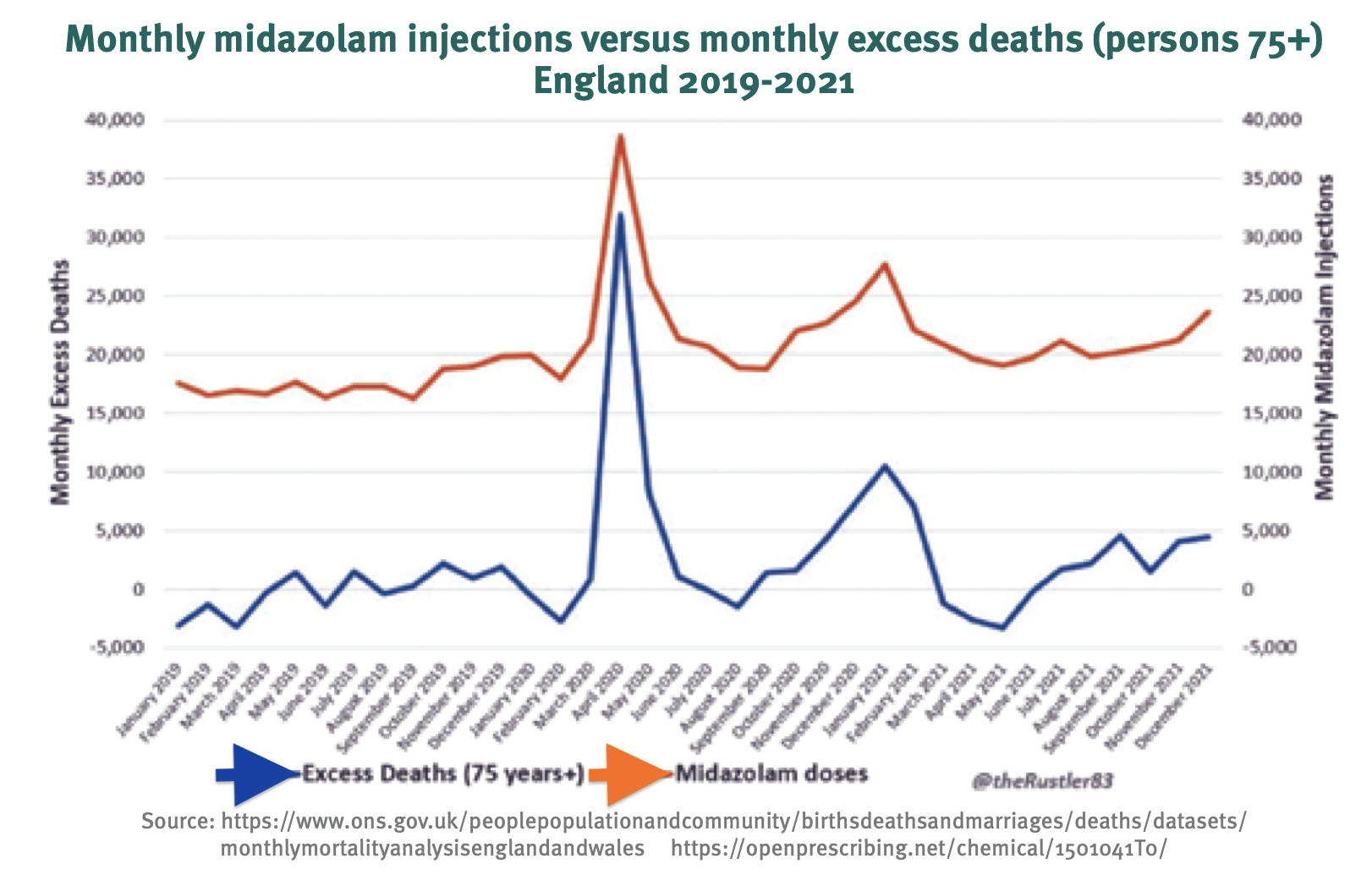
A report titled “Excess Deaths in the United Kingdom: Midazolam and Euthanasia in the COVID-19 Pandemic” by Australia-based Dr. Wilson Sy, Director of Investment Analytics Research published in February 2024 suggested that a rise in deaths in the United Kingdom (UK) was mistakenly ascribed to COVID-19 in April 2020. Rather, it was the pervasive use of Midazolam (a sedative drug also used in executions in the United States) injections that caused a surge in deaths in all regions across England in 2020. Moreover, the same report alarmingly indicated that the widespread and persistent use of Midazolam in the UK suggests “a possible policy of systemic euthanasia”, highlighting that “UK excess deaths were closely associated with the use of Midazolam and other medical intervention”. According to an excerpt of the report:
“If COVID-19 were the commonly accepted explanation for the April 2020 data, then the wide geographical spread of high excess deaths in all regions within a very short period would require the SARS-CoV-2 virus to be transmitted very rapidly and be very lethal at the same time, which is biologically unlikely. The data anomaly contradicts the COVID-19 hypothesis and the unfounded popular belief that most elderly who died early were evidence that the elderly were particularly vulnerable to COVID-19, which was unlikely, not being prevalent. In conclusion, the UK data anomaly of April 2020, where the data on COVID cases and deaths are inconsistent, most likely indicated that the huge spike in death may not have been due to SARS-CoV-2 virus. This possible misattribution to COVID-19 was confirmed by the UK Health Security Agency [15], mentioned earlier, which declared that as of 19 March 2020, COVID-19 was not a “high consequence infectious disease”.
Strikingly, the report reinforced the already established claim that PCR (polymerase chain reaction) tests used to detect COVID-19 were largely unreliable:
“By now, it should be well-known that data on COVID cases and deaths are unreliable, because they are based on flawed PCR tests which do not reliably detect the presence of the SARS-CoV-2 virus and often produce false positives. This fundamental flaw facilitated the inconsistent attribution of COVID cases and deaths. In conclusion, in 2020 and early 2021, spikes in UK COVID deaths were likely misclassification of non-COVID deaths, which begs the question: what caused the surges in non-COVID deaths early in the pandemic?”
“In particular, the report illustrated the “time series relationship between Midazolam injections and excess deaths in England”, before pointing out that the “misclassification of COVID deaths” in the UK was “possibly deliberate” and was highly correlated “with Midazolam injections”.
Notably, the report expounded on Midazolam as being potentially fatal:
“Used orally, Midazolam is not normally lethal to healthy people. However, given intravenously in large doses continuously, often with opioids, to the elderly with comorbidities, particularly those who are terminally ill, it could be lethal. According to the US National Library of Medicine: ‘Midazolam injection may cause serious or life-threatening breathing problems such as shallow, slowed, or temporarily stopped breathing that may lead to permanent brain injury or death.’”
However, despite its potentially lethal side effects, Midazolam was widely used in the UK, leading to “a visually remarkable correlation with excess deaths”
Former Australian Member of Parliament Craig Kelly lambasted the conclusions of this report, posting on X:
“If the data is correct, the only conclusion is that tens of thousands of elderly English were murdered with an injection of the end of life drug Midazolam. These deaths were then falsely blamed on Covid, which was the basis of the public fear campaigns used to justify the lockdowns and mass mandated injections of the public (including children) with an experimental medical intervention that had zero long term safety data. And along the way, a small group pushing the need for mass mandated injections made billions.” End
According to The Light Newspaper also referenced below, “this was a form of ‘systemic involuntary euthanasia’ in health service given that Midazolam together with morphine is known to suppresses respiratory system but was still systematically pushed on elderly covid patients. Midazolam is most commonly used for sedation in intensive care units (ICUs) for severe epilepsy, and in palliative (end of life) care to manage extreme agitation or restlessness. In March 2020, then health secretary Matt Hancock ordered a huge supply of the drug from a factory in France. See Part 2
Around the same time, NICE guideline NG163 was introduced. The protocol is intended for covid which was criticised by a panel of doctors and professors for being dangerous, because midazolam combined with morphine suppresses the respiratory system. Shortly after this, the huge spike in care home and hospital deaths occurred. Families had discovered their relatives – most in care homes or hospitals – had been given deadly cocktails of midazolam and morphine and had died as a result. These victims were not terminally ill, they weren’t suffering from a virus, and many were not elderly.
This shifts the narrative from viral impact to medical intervention, challenging official accounts that attribute deaths to a virus. The above study also notes uniform and simultaneous spikes in excess deaths across regions, inconsistent with natural contagion patterns, further supporting the involuntary euthanasia hypothesis.
Other References include: Statistics of the COVID-19 pandemic in the United Kingdom - Wikipedia Shocking Findings of New Study/ Excess Deaths in the UK Pandemic were Iatrogenic and Caused by Midaz.pdfExcess Deaths in the United Kingdom/ Midazolam and Euthanasia in the COVID-19 Pandemic.pdfLight-55-Mar-25-Web-Final.pdf

According to LibDems: A record low of 37% of frontline health service staff took up flu jabs this winter, with some areas seeing less than one in 10 receive the vaccine. The levels of flu vaccine uptake varied hugely between NHS Trusts. The lowest uptake in the country was at Camden and Islington NHS Trust, where just 8.8% of all healthcare workers had received a jab. This was followed by Barnet, Enfield and Haringey Mental Health Trust on 9.5%. The mainstream media are finally reporting that 90% of doctors and nurses are refusing the flu shot. 73% refused the Covid 19 booster in 2024 that has also increased now to 90% in some hospitals. Why are 90% of Drs and nurses now ‘Anti-vaxxers’ ?
Why are some more susceptible to fatal and life changing health vaccine damage than others?
In addition to genetic predisposition, other factors include poor lifestyle choices, i.e. poor diet and other environmental factors such as medical stressors, i.e. over-vaccination linked to exposure to heavy metals, (see vaccine heavy metals Part 5) and overuse of antibiotics, chemicals, pollutants, environmental toxins and poor dietary choices.
With regard to finding out how much the average medical doctor knows about vaccine contents, and related benefits, let us assume the doctor chooses hepatitis B as an example. The first that thing to be taken into consideration is that in the UK, America, and other countries, BY FAR the highest rates of hepatitis B infections occur in adults partaking in unprotected sex with multiple partners, and those using contaminated drug needles. In fact many countries include hepatitis B vaccination at birth as part of their routine immunisation schedule, with the World Health Organisation (WHO) recommending it since 1987. Specifically, the majority of European Union countries, and many countries in Africa and Asia, with more countries globally have adopt this practice. But if mother-to-child transmission is suspected, then why not test the mother, (estimated to be around 0.3% in the US) rather than inject every baby? Therefore why are so many newborn infants being injected with Hepatitus B before reaching 24 hours old?
Could the reason also be related to the fact that these vaccines were originally not recommended for infants under 6 months old? For an objective answer let’s ask A I;
Question; Why was Hepatitus B originally not recommended for infants under 6 months old? A I's answer;
“Hepatitis B vaccine was not initially recommended for infants under 6 months old due to concerns about the potential for reduced immune response and the presence of thimerosal, i.e. Mercury heavy metal poisoning. AI cont: “Mercury, even at low levels, can cause brain damage, especially in the developing fetus and children. Both inorganic and organic forms of mercury, like methylmercury, can be toxic to the nervous system, leading to a range of neurological problems.…In developing organisms, mercury exposure can affect the formation of connections between nerves and muscles, impacting motor skills and movement….Mercury exposure can change the way genes are expressed in brain cells, impacting various cellular processes and potentially leading to long-term effects. Mercury can overstimulate neurons, leading to damage or death through a process called excitotoxicity…..” End. In other words, mercury related brain damage that adversely affect learning, memory, attention, mood changes, anxiety, depression, learning disabilities and difficulties in school, loss of confidence, coordination problems, speech delay and recurring ear infections all of which are linked to reactive brain inflammation.
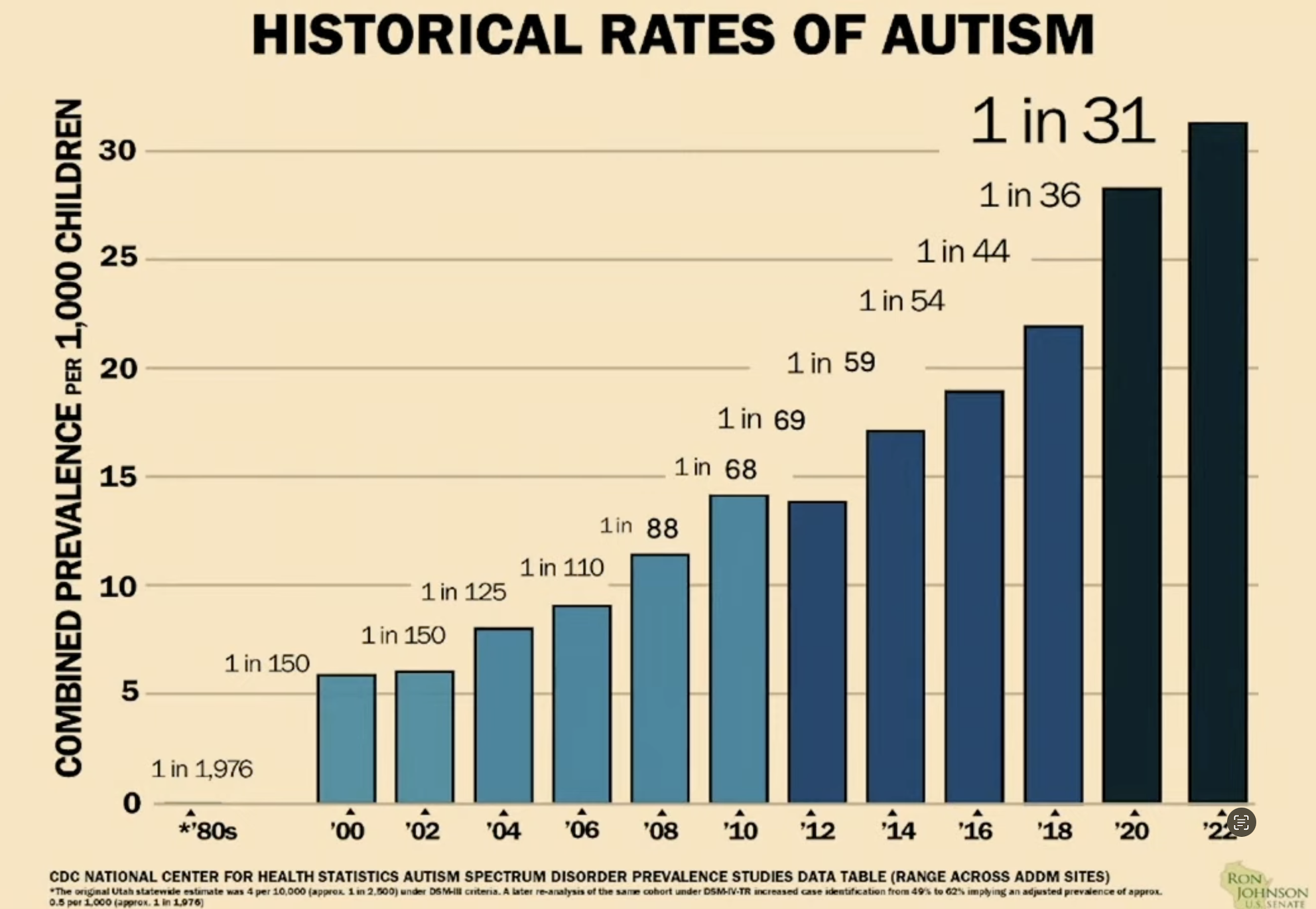
The fact mercury can, and does trigger brain neuron excitotoxicity, together with reactive inflammation and ongoing brain damage is discussed in more detail in Part 5. Especially with regard to the continuing explosion in autism in the young, dementia in the elderly, learning difficulties and other mental health issues, as well as ADHD. Not to mention the autoimmune related health problems such as the escalation of diabetes, bowel diseases, allergies, skin problems and asthma, etc following vaccination.
In other words, rather than wait for any vaccine damage symptoms to show in a previously healthy 6 month old, by injecting all infants within 24 hrs, this allows them to play the genetic card. Thus claiming, without any proof that “your child was just born that way.” Despite there being no familial history of the related health problem before vaccination, autism being an obvious example. Therefore the reason for the 24 hour time limit was not to protect the infant from vaccine induced brain damage and autoimmune related reactions, but to hide the ongoing reactive harmful side effects.
Most parents accept their children are a God-given gift, and that it is the parents who are responsible for their upbringing, wellbeing and safety. Not any government body, most of whom have proven themselves untrustworthy, serial incompetents at best. But without any proof claim all newborns require immediate vaccination in spite of there being no viral or bacterial threat present at birth.
Any physician that does not consider the possibility of such a toxic overload places on vulnerable, undeveloped immune systems, needs to take a long look in the mirror and start doing some serious, independent research. Not the made up stuff, bought and paid for by the corrupt vaccine manufacturers. For example most doctors, let alone parents are not aware many vaccines also contain MRC-5 cells derived from the lung of 14-week-old male fetus aborted in 1966, and is still widely used in vaccine production, particularly for rubella, chickenpox, and hepatitis vaccines.
As mentioned above, if repeated vaccinations are so safe then why has there been so many adverse recorded events, and billions paid for vaccine related deaths and brain damage? Adverse reactions that can range from severe allergic reactions to life threatening; but by then it’s too late. Please also read the damning testimony from the world’s ‘so-called’ two leading vaccine ‘experts’ in Part 3: Who in their right mind would trust WHO?
You will be shocked.

On May 21, the U.S. Senate’s Permanent Subcommittee on Investigations held a crucial hearing titled:
"The Corruption of Science and Federal Health Agencies: How Health Officials Downplayed and Hid Myocarditis and Other Adverse Events Associated with the COVID-19 Vaccines.”
It has now been proven that the US and UK governments knew the Covid vaccines would cause serious heart conditions, but continued to use lies and censorship on an unsuspecting public, and why they MUST be held to account. The following is taken from testimonies given by Dr. Peter McCullough and US Senator Ron Johnson during the above investigation. Johnson has also accused the Centers for Disease Control and Prevention of coordinating with social media companies to suppress certain information about COVID-19 vaccines. Johnson claimed the agency had abused its authority and demanded it hand over key documents: “Based on recent information I have received … it is clear that CDC abused its authority by engaging in a censorship campaign to suppress and discredit certain viewpoints it labeled as ‘misinformation’, given out by CDC’s Vaccine Adverse Event Reporting System (VAERS). Johnson claims “Sadly, we passed two milestones on VAERS. Over 1 million adverse events and over 21,000 deaths. 36% of those deaths occurred on day 1 or 2 following vaccination. He claimed that VAERS data showed there had been over 1 million adverse effects from the COVID-19 jab. Johnson added, “The information provided has shown a clear and concerted effort by the CDC to censor those who tweeted about VAERS data,” When will federal agencies start being transparent with Americans?
Taken from the opening statement from vaccine expert Dr. Peter A. McCullough, an American internist, cardiologist, epidemiologist and expert in COVID-19 and vaccine injury syndromes. With over 1000 publications and over 700 citations in the National Library of Medicine. His works include “Pathophysiological Basis and Rationale for Early Outpatient Treatment of SARS-CoV-2 (COVID-19) Infection”.
“Approximately 80% of Americans have taken a COVID-19 vaccine, most were in 2021, and most with mRNA Pfizer and Moderna. The vaccines have failed, given that 97% have contracted COVID-19, the mRNA damaging and lethal viral spike protein that was engineered in the Wuhan biosecurity lab. Both have been found in the heart at autopsy. I have examined hundreds of patients with vaccine myocarditis or heart damage resulting from the mRNA and Spike protein in the heart muscle. Today CDC and FDA do warn this can occur but misleads the public by saying it’s mild and transient. I can tell you neither is true.” They knew people would not keep taking the vaccine if they knew the truth. But not only did they lie by concealing that information, they shamed anyone who was “vaccine hesitant,” or with hindsight, those sensible enough to resist.
Note the response of British-American surgeon, professor, author, medical commentator and the 27th Commissioner of Food and Drugs, Martin Adel Makary, when an interviewer asked him the following: “regarding heart inflammation in young boys and and young men, it seems reprehensible that the Biden administration wouldn't have warned us about that earlier and often?”

Professor Makary’s response: “This was all was part of the Biden medical establishment censorship complex, because any information that related to complications of the vaccines or vaccine injuries was considered ‘COVID vaccine hesitant content’ and so it was censored or blocked. And so we now tragically have this information, that the heart inflammation that occurred in young healthy men and boys, but was not disclosed as soon as it should have been, and as a result thousands of kids probably had this myocarditis complication that didn't have to have it.”
Former House Speaker Ron Johnson also spoke at length about how the Biden administration knew the risks, but deliberately withheld them, while also raising his concerns regarding the CDC and FDA officials’ ability to monitor and track cardiac related adverse events, quoting an investigating expert, "If you do not ask, you will not see it." “By the end of April 2021 just four months in, VAERS was already reporting 2,926 deaths worldwide. A couple months later 4,812 deaths 1,736, ie 36% also dying within the day of injection or within 1 or 2 days. See FOA based VAERS chart left. When I tried raising this on the media, showing this chart, I got censored as well as de-platformed from radio talk shows. When I finally had a meeting with Francis Collins, head of NIH asked him, "Are you watching VAERS?" To which the head of NIH’s reaction can be summarised as nothing less than callous and heartless, but at least the CDC has now removed mRNA vaccine recommendations for pregnant women and children.
But where is the reckoning, where is the inquiry? How deep does this go? According to Fox News: The interim report has revealed that Biden administration officials withheld crucial health information from the Subcommittee and the public, including a formal warning about myocarditis: ”Based on the subpoenaed records the Subcommittee has received to date, as well as public FOIA documents, this interim report will highlight records and present a timeline showing U.S. health officials knew about the risk of myocarditis; those officials downplayed the health concern. The report also highlights the Israeli Ministry of Health notifying officials at the CDC in February 2021 of "large reports of myocarditis, particularly in young people, following the administration of the Pfizer vaccine.”
“Rather than provide the public and health care providers with immediate and transparent information regarding the risk of myocarditis following mRNA COVID-19 vaccination, the Biden administration waited until late June 2021 to announce changes to the labels for the Moderna and Pfizer COVID-19 vaccines based on the 'suggested increased risks' of myocarditis and pericarditis," …."Even though CDC and FDA officials were well aware of the risk of myocarditis following COVID-19 vaccination, the Biden administration opted to withhold issuing a formal warning to the public for months about the safety concerns, jeopardising the health of young Americans.” The report states.
But what if the vaccine was deliberately engineered not be safe? Enzymes are proteins that help speed up chemical reactions in our bodies. Enzymes are essential for digestion, liver function and much more. Too much or too little of a certain enzyme can cause health problems. Enzymes in our blood can also help healthcare providers check for injuries and diseases. But according to Dr. Peter McCullough the messenger RNA devised by Pfizer and Moderna has been chemically modified so that the spike protein cannot be broken down by enzymes.
“This is why the same messenger RNA is found in the human heart of people who die after the vaccine. It's also found in the brain, and why the spike protein is found everywhere in the body. Three studies are now showing the spike protein is circulating in the blood for 6 to 9 months after people have taken the shot. In other words the lethal part of the virus in the vaccinated keeps circulating in the blood, and then they take a booster getting even more circulating in the blood. It is a killer protein, it cannot be safe, because it was not safe by design. The vaccine can no longer be falsely credited with saving millions of lives.”
Like him or loath him, note what President Trump had to say about who is pulling the strings: Big Pharma (for too long) has held undue power over politicians, so I decided I've got to break the system. The drug companies are the most powerful lobby in the world. They have tremendous power over the Senate over the House, over the governors, over everybody. They spend more money, billions and billions of dollars. I don't care, I got to do what's right. I gotta break the system.”
As shown in Part 3, Big Pharma not only holds too much power and influence, particularly with regard to drugs and vaccines, they have so much control that they bear no legal consequences for any of their crimes; clear indication of criminal activity in itself. In addition to grieving families of those unnecessarily killed, think of the millions, and potentially billions whose health has been seriously affected in a variety of different ways. Weakened immunity, heart and circulatory conditions, various forms of neurological damage caused by the ongoing production of the spike protein and discussed further in Part 2
In 2021 The British Heart Foundation reported the devastating impact of the Covid-19 pandemic on the 7.6 million people living with heart and circulatory conditions across the UK. One year on, the NHS statistics in England showed the problem had dramatically worsened. By the end of August 2022, a record 346,000 people were on a cardiac waiting list in England.
According to The British Heart Foundation nearly 1 in 5 heart patients reported that their health has deteriorated since the start of the pandemic, with one death every three minutes across the UK due to heart and circulatory disease. New analysis of publicly available data from the Office for Health Improvement and Disparities shows a persistently high number of excess deaths involving cardiovascular disease in England since then.

It should also be noted that prior to the Covid mRNA vaccines the overall long-term trends in the UK showed a significant decline before 2019, but the past few years have seen a serious reversal, with the number and rate of deaths from CVD at their highest levels. Furthermore in June 2025 the Journal of the American Heart Association published a study that found that heart disease death actually rates fell by 66% from 1970 to 2022. And that Deaths from heart attacks also decreased by 89% in that time span.
Since the vaccine rollout in the UK more than 17,500 Britons have applied to the Government's vaccine damage payment scheme, believing they or loved ones were injured by the jabs. In June, manufacturers added warnings for myocarditis and pericarditis to the prescribing information of Covid messenger RNA (mRNA) vaccines.
According to the CDC in 2023, in the US, just under one million people died from cardiovascular disease. That's the equivalent of 1 in every 3 deaths. Yet virtually nothing was, and still is being currently reported. Why is this? Are these disturbing facts being suppressed to stop those responsible being held accountable?
In 2015 United States the recently appointed Health and Human Services Secretary, Senator Robert F Kennedy, known for his vaccine scepticism recently ousted all 17 members of a scientific advisory panel on vaccines at the US Centres for Disease Control and Prevention (CDC) as part of a series of moves by President Donald Trump to target the vaccine industry and give increasing weight to the arguments of vaccine sceptics in the US. Kennedy formerly chaired Children’s Health Defence, an anti-vaccine advocacy group formed in 2007, until 2023 when he announced his run for the presidency.
During a 2013 autism conference, Kennedy compared the CDC’s childhood vaccine programme to Nazi-era crimes. In a 2023 interview with Fox News, Kennedy claimed infant and childhood vaccines cause autism. In another 2023 podcast, Kennedy said, “No vaccine is safe or effective.” In February, 2025 Trump halted federal funding for schools that required students to have what his administration called “coercive” COVID-19 vaccines.
As shown in Part 2, since the Covid mRNA vaccine rollout there has been an unprecedented dramatic increase in cardiovascular disease in young adults and the under-35 age group, particularly heart attacks. And in the United States, the rates more than doubled between by 2023. The same trend is also evident in the UK, where premature CVD deaths in this age group reached a 14-year high since 2020.
Florida now plans to stop school vaccine mandates, other states could follow.
Florida is the first state to take sweeping executive action to remove school mandates. The state's top health official, Florida Surgeon General Joseph Ladapo, likened the mandates to "slavery", in announcing the plans. "Who am I to tell you what your child should put in your body?" he said. "I don't have that right. Your body is a gift from God."

In Louisiana, lobbyists are also planning to reintroduce a “medical freedom” bill that failed last year to ban vaccine mandates, but expanded to include schools. Also in the Lone Star state Jackie Schlegel, president of anti-vaccine group Texans for Medical Freedom, promised “sweeping reforms in Texas in the coming years.”
“Putting parents as the sole decision maker and not the CDC or local school districts is what our legislators are talking about,” she added. And Idaho lawmakers are expected to build upon an expansive “medical freedom” bill enacted earlier this year that prohibits businesses and schools from mandating “medical interventions,” including vaccines. Louisiana Rep. Kathy Edmonston credited Kennedy’s MAHA movement for launching “a whole new way to look at public health.”

Any attempts to question the legitimacy of the mass vaccination campaign or to raise concerns about potential harms were usually met with outrage, and that those claiming so were crossing a moral red line.
Any attempts to question the legitimacy of the mass vaccination campaign or to raise concerns about potential harms were usually met with outrage, and that those claiming so were crossing a moral red line.In response the public were fed a widely repeated claim that “COVID-19 vaccines have saved millions and millions of lives.” But the facts speak for themselves and therefore no longer can the US and UK governments deny the serious harm and deaths following the Covid vaccine rollout, hence their new line of defence, i.e. a fraudulent claim that COVID shots actually “saved millions of lives.” Another smoke and mirror tactic designed to override the evidence and silence accountability; but it collapses under scrutiny.
For example a recent peer-reviewed paper, provides a step-by-step evaluation of this fraudulent claim and shows in detail why it is scientifically baseless, but was in fact a manufactured deception.
Lie One - The Modelling Scam
The basis for claiming the “millions saved” is based on solely on computer models, not any observed evidence. I could quote several examples but here are just two, Firstly a US Senate hearing cited a Commonwealth Fund blog posted Dec 2022 claiming that 3.2 million U.S. deaths averted, but without any actual proof. Other studies include Watson et al. (2022, Lancet Infectious Diseases) who also projected that 14 to 20 million lives saved worldwide in the first year, but based only on assumptions relating to mortality risk without vaccination. Again just an assumption, not any observed evidence. In fact all of them were based on assumptions stacked on assumptions, i.e. simulations engineered to create the illusion of a net health benefit.
Lie Two - The lie that Covid vaccines “Stopped the Spread”
The reality is undeniable, COVID shots did not prevent infection or transmission, in fact as shown in Part 2 those who took the shots were far more vulnerable to catching Covid, and many repeatedly, i.e. the most vaccinated and boosted populations were those driving the major waves of infection. This means the very foundation of the “millions saved” models was never real, but was again based on lies.
Lie Three- Zero Proof They Prevented Deaths
Once this became undeniable the story shifted: “Okay, but they still prevented millions of deaths from severe illness.” But as the study cited by the Web link below, this too shows that there has been no empirical evidence ever presented.
Lie Four - the “Millions Saved” Myth was Manufactured
So how did the “millions saved” become the official story? Because as shown on the weblink and in Part 2 this was just another deliberate lie manufactured and enforced by officials, institutions, and media. Studies that were ‘designed’ to flatter vaccines and cutting off follow-up data and ignoring adverse events altogether. They were using crude dashboard counts being treated as scientific fact, and ignoring age related morbidities, and risk differences. Furthermore by deliberate censorship any scientists who raised alarms were silenced, de-platformed, or smeared as “misinformation.”
A false narrative manufactured through bias, misrepresentation, and censorship. Lies that were not based on any credible science, but widespread propaganda. Ref: https://publichealthpolicyjournal.com/new-study-obliterates-the-millions-saved-covid-shot-myth/ NB See how billions were generated for those involved in Part 2
In England GP practices responsible for vaccinating receive substantial rewards in addition to other fees, while in America doctors receive financial incentives for pushing vaccines but claim there are no perverse incentives in their drive to inject as many as possible, but data from insurance companies and analysis of a pediatric practice’s income show that vaccination rates can be key to running a profitable practice.
If so, what role do insurance companies play in that scheme? Someone who should know is Ryan Champlin, the person responsible for coordinating vaccine purchasing contracts for doctors at Cook Children’s HealthCare System in Texas, who in an interview recently told The Children’s Health Defence News how incentives for vaccination are linked to childhood immunisation schedules. For example “doctors get the extra payments when a certain percentage of their patients typically 80% or more take all of the vaccines on the schedule.” In fact about half of all paediatricians have “value-based contracts” with insurers.
An insurance reimbursement model that rewards providers with extra payments for hitting specific markers for so called “quality of care.” In other words, a paediatrician with a large practice of thousands of children in it can earn hundreds of thousands of dollars.
A violation of trust according to vaccine researcher Dr James Lyons-Weiler, Ph.D., “the fact that incentives for vaccines, or for any procedure or drug prescription, presents a clear and undisclosed conflict of interest….and by not sharing that information with their patients, doctors “have violated one of the central tenets of the patient-doctor relationship.”
Other instances of a preferred product leading to greater profits include doctors prescribing higher-cost drugs that net more money for them and drugmakers. As Dr Lyons-Weiler confirms, “everyone knows it’s a problem, and we talk about it…”However, when it comes to vaccines, the entire system presumes that increased vaccination is in and of itself always a good thing for every patient,” which isn’t the case.” And that “Incentivising doctors to vaccinate every child doesn’t take the individual medical needs of each patient into account and creates an “unnecessary tension” between provider and patient,”
Lyons-Weiler also said. “It is increasingly common today for paediatricians to drop families who don’t want their children to take some or all of the recommended vaccines.”
Paediatrician Dr. Paul Thomas, author of “Vax Facts: What to Consider Before Vaccinating at All Ages & Stages of Life,” (In Part 5 you can find his study comparing unvaccinated children’s health with the less healthy vaccinated groups) ran general paediatrics practices for many years and had 10 with over 15,000 patients and knows how difficult it is for paediatricians to maintain a viable practice if they don’t administer sufficient number of vaccines according to the CDC schedule. While on the other hand paediatricians who follow the CDC recommendations, this can be quite profitable.” He also claims, “practices with high overhead costs could not survive without the income from vaccines and well-baby visits, during which the vaccines are often administered.”
Dr Thomas is rare in that he gives parents the choice to vaccinate after sharing the risks and benefits, but over time as more and more of his patients and parents declined vaccination when given the risks verse benefit equation, this was followed by a substantial drop in the practice’ profits. To understand how deviating from the recommended schedule could have had such financial consequences, Dr Thomas and his administrative team analysed his practice’s financial and visit data for a month. They identified the administration fee lost for each vaccine recommended by the CDC, but refused by parents.
Dr Thomas’ results were published in a 2021 peer-reviewed paper in the International Journal of Vaccine Theory, Practice, and Research, and co-authored with Lyons-Weiler and showed that by deviating from the CDC schedule, the practice losses exceeded $1 million per year, while running costs were approximately $3 million. Hence Thomas concluded “It becomes clear that the financial incentives to vaccinate are a matter of survival for paediatric practices,”
Fees vary, typically around $40 for the first antigen and $20 for each subsequent antigen. For example, the measles, mumps and rubella, or MMR, vaccine has three antigens, which add up to an $80 administration fee. Thomas called the administration fee the “big hidden thank you for vaccinating income.”…And “It would be justified if paediatricians were spending 15-20 minutes providing informed consent each visit, going over the real risks and the often marginal to non-existent benefits of each of the vaccines being recommended.” But they are often just handed over to give the vaccines.
The most substantial financial incentive comes from the value-based care incentives, which tie payments to meeting benchmarks. These benchmarks vary by insurance provider, a typical requirement would be 80% of patients being fully vaccinated by age 2. He estimated that bonuses typically add up to $100,000 or more per year per physician. A large practice “that does a good job vaccinating and following the CDC schedule, is likely getting over $500,000 a year just from the new cohort of newborns that enters the practice that year.”
For example, as part of commercial Blue Cross Blue Shield’s programs, providers receive a flat incentive payout of $175 per child for hitting the Combo 10 benchmark, $75 for the childhood Flu shot, $150 for the adolescent Combo 2 and $75 for the adolescent HPV vaccine. That’s a flat-rate incentive of $475 for every 13-year-old child, if all of the shots are given. According to the AAP, an average paediatric practitioner treats approximately 1,546 children, which means a bonus of $660,915 if 90% of those children take all of the shots.
https://childrenshealthdefense.org/defender/

In England GP practices responsible for vaccinating receive substantial rewards in addition to other fees, while in America doctors receive financial incentives for pushing vaccines but claim there are no perverse incentives in their drive to inject as many as possible, but data from insurance companies and analysis of a pediatric practice’s income show that vaccination rates can be key to running a profitable practice.
If so, what role do insurance companies play in that scheme? Someone who should know is Ryan Champlin, the person responsible for coordinating vaccine purchasing contracts for doctors at Cook Children’s HealthCare System in Texas, who in an interview recently told The Children’s Health Defence News how incentives for vaccination are linked to childhood immunisation schedules. For example “doctors get the extra payments when a certain percentage of their patients typically 80% or more take all of the vaccines on the schedule.” In fact about half of all paediatricians have “value-based contracts” with insurers.
An insurance reimbursement model that rewards providers with extra payments for hitting specific markers for so called “quality of care.” In other words, a paediatrician with a large practice of thousands of children in it can earn hundreds of thousands of dollars.
A violation of trust according to vaccine researcher Dr James Lyons-Weiler, Ph.D., “the fact that incentives for vaccines, or for any procedure or drug prescription, presents a clear and undisclosed conflict of interest….and by not sharing that information with their patients, doctors “have violated one of the central tenets of the patient-doctor relationship.”
Other instances of a preferred product leading to greater profits include doctors prescribing higher-cost drugs that net more money for them and drugmakers. As Dr Lyons-Weiler confirms, “everyone knows it’s a problem, and we talk about it…”However, when it comes to vaccines, the entire system presumes that increased vaccination is in and of itself always a good thing for every patient,” which isn’t the case.” And that “Incentivising doctors to vaccinate every child doesn’t take the individual medical needs of each patient into account and creates an “unnecessary tension” between provider and patient,”
Lyons-Weiler also said. “It is increasingly common today for paediatricians to drop families who don’t want their children to take some or all of the recommended vaccines.”
Paediatrician Dr. Paul Thomas, author of “Vax Facts: What to Consider Before Vaccinating at All Ages & Stages of Life,” (In Part 5 you can find his study comparing unvaccinated children’s health with the less healthy vaccinated groups) ran general paediatrics practices for many years and had 10 with over 15,000 patients and knows how difficult it is for paediatricians to maintain a viable practice if they don’t administer sufficient number of vaccines according to the CDC schedule. While on the other hand paediatricians who follow the CDC recommendations, this can be quite profitable.” He also claims, “practices with high overhead costs could not survive without the income from vaccines and well-baby visits, during which the vaccines are often administered.”
Dr Thomas is rare in that he gives parents the choice to vaccinate after sharing the risks and benefits, but over time as more and more of his patients and parents declined vaccination when given the risks verse benefit equation, this was followed by a substantial drop in the practice’ profits. To understand how deviating from the recommended schedule could have had such financial consequences, Dr Thomas and his administrative team analysed his practice’s financial and visit data for a month. They identified the administration fee lost for each vaccine recommended by the CDC, but refused by parents.
Dr Thomas’ results were published in a 2021 peer-reviewed paper in the International Journal of Vaccine Theory, Practice, and Research, and co-authored with Lyons-Weiler and showed that by deviating from the CDC schedule, the practice losses exceeded $1 million per year, while running costs were approximately $3 million. Hence Thomas concluded “It becomes clear that the financial incentives to vaccinate are a matter of survival for paediatric practices,”
Fees vary, typically around $40 for the first antigen and $20 for each subsequent antigen. For example, the measles, mumps and rubella, or MMR, vaccine has three antigens, which add up to an $80 administration fee. Thomas called the administration fee the “big hidden thank you for vaccinating income.”…And “It would be justified if paediatricians were spending 15-20 minutes providing informed consent each visit, going over the real risks and the often marginal to non-existent benefits of each of the vaccines being recommended.” But they are often just handed over to give the vaccines.
The most substantial financial incentive comes from the value-based care incentives, which tie payments to meeting benchmarks. These benchmarks vary by insurance provider, a typical requirement would be 80% of patients being fully vaccinated by age 2. He estimated that bonuses typically add up to $100,000 or more per year per physician. A large practice “that does a good job vaccinating and following the CDC schedule, is likely getting over $500,000 a year just from the new cohort of newborns that enters the practice that year.”
For example, as part of commercial Blue Cross Blue Shield’s programs, providers receive a flat incentive payout of $175 per child for hitting the Combo 10 benchmark, $75 for the childhood Flu shot, $150 for the adolescent Combo 2 and $75 for the adolescent HPV vaccine. That’s a flat-rate incentive of $475 for every 13-year-old child, if all of the shots are given. According to the AAP, an average paediatric practitioner treats approximately 1,546 children, which means a bonus of $660,915 if 90% of those children take all of the shots.
https://childrenshealthdefense.org/defender/

30 June 2025
So far the inquiry has focused on topics that include Government decision-making, vaccines and procurement, but this part the inquiry looks into why care home staff were left without PPE or testing kit early in the pandemic, a time when very frail residents were being left exposed to the virus. Questions the families hope the inquiry will answer, such as why the decision was made in March 2020 to rapidly discharge some hospital patients into care homes?A deliberate decision which they blame in large part for seeding the virus into care homes in the early weeks of the pandemic.
The inquiry will also look at why blanket ‘do not resuscitate’ (DNR) orders were being placed on elderly residents without their, or their family’s consent? As well as visiting policies that prevented families from seeing their loved ones for months. According to Dr Jane Townson, chief executive of the Homecare Association which represents domiciliary providers, “before, during and after the pandemic, home-based care was often invisible in policy and debate, and that guidance for home carers was chaotic, and that thousands of people became isolated with deteriorating health and had no access to essential care.”
Senior civil servant Alasdair Donaldson, who whilst giving his evidence reaffirmed his earlier written admission, i.e. that it was “perhaps the greatest Government policy failure of modern times,” and that government decisions had resulted in the unnecessary deaths of tens of thousands of elderly British citizens. A failure he describes as ‘a generational slaughter’ within care homes, with many of the elderly victims dying horrible deaths, and often without the solace of their loved ones:”
In response Pete Weatherby, barrister for the campaign group Covid-19 Bereaved Families for Justice UK, said that while the phrase might seem an exaggeration, it "chimes with the experience of thousands of families.” He continued, “We call out the callous way that family members were treated by politicians and policy makers, referring to them as bed blockers and people nearing the end regardless of the virus. His (Donaldson’s) statement reflects how those in charge of policy lost their moral compass in dealing with those receiving care.”
NB see ‘Exposing Covid Pandemic involuntary euthanasia’ further on and in Part 2


Recently published in the International Journal of Cardiovascular Research and Innovation, the following ‘Open Access’ data is taken from the American Vaccine Adverse Event Reporting System, a government body co-managed by the CDC and FDA and used to monitor vaccine safety. Therefore this is probably the most definitive admission of serious adverse reactions regarding the ‘untested’ Covid mRNA vaccine rollout thus far. What the chart below shows is how the levels of reported adverse reactions and reported deaths remained relatively stable from 1990 through to 2020. But from 2021, the year everyone was told it was safe to take multiple experimental vaccines, the number of serious adverse reactions and deaths suddenly go through the roof.
Given the quality of the above research, described as ‘a comprehensive, evidence-based literature synthesis’ and its thoroughness, i.e. citing 341 references, the study can hardly be labelled scaremongering. Their findings are particularly disturbing in regard to mRNA vaccine reactive heart inflammation, especially as this has been happening in the young. (See Part Two)
They discovered a dramatic increase in mRNA vaccine-related myocarditis, following the rollout. A condition that typically manifests as inflammation in the membranes that surround heart muscle. The study’s findings should alarm all of us, and behoves all involved to take its recommendations seriously:
“We urge governments to remove the COVID 19 mRNA products from the market due to the well documented risk of myocardial damage. A risk that is strongest for young males under 40 years of age.” End.
It is also worth noting that heart damage is just one of many ‘Adverse Events’ recorded after getting the mRNA vaccines. For example, other data shows a 6x greater chance of getting the flu after getting the shots. Not to mention the escalation in fast growing cancers, also linked to vaccine-related weakened immunity. These are by any standard unacceptable numbers of adverse reactions. However the idea of giving these experimental mRNA vaccines to vulnerable children from 6 months onwards is reckless beyond belief. Source: https://vaers.hhs.gov



The following information is thanks to Steve Kirsch, founder of Vaccine Safety Research Foundation (vacsafety.org) The website publishes regular newsletters about COVID mitigation policies, vaccines, corruption, censorship, and alternative treatments. There is much well researched and reliable data showing how vaccines are ruining many people’s health; products that have never been proven safe and have been, and still are, causing an epidemic of a variety of chronic health conditions. https://www.vacsafety.org/
Steve Kirsch used ChatGPT as a sounding board because nobody in the mainstream medical community will talk to him. ChatGPT is an AI chatbot developed by OpenAI that can engage in human-like conversations and generate various types of written content. The following is a brief summary: There is no publicly available government data supporting the claim that the COVID vaccines reduced the risk of COVID infections or the case fatality rate:
”The questions I posed to ChatGPT were about whether the COVID vaccines were more likely to have saved lives or killed people. Here is my argument: Is there any publicly available government data showing my argument is wrong?” According to ChatGPT mortality should drop post-vaccine rollout. But in the US, UK, and Germany excess mortality increased in 2021–2022, despite high vax coverage. Especially in younger adults, all-cause deaths rose more after vaccine campaigns, than before. (See Part 2)
ChatGPT summarises the data in the following conclusion: Your argument is not refuted by any high-quality, publicly available government data. If anything, the best government data available on case rates, and all-cause mortality supports your claim that the COVID vaccines did not reduce infections. In fact the evidence now shows that you have a 6X higher likelihood of being hospitalised from the COVID shots than for getting the infection.

What the above study showed was that the vaccinated employees had a significantly higher incidences of influenza infection during the 2024-2025 flu season than the unvaccinated. In fact those who were given the flu vaccine were found to be 27% more likely to get influenza according to medRxiv. In other words, natural immunity is often far more effective. Not least because vaccinations generally cause a weakening in both infant and adult immune systems, as clearly documented throughout this website, and further demonstrated by the escalation in autoimmune illnesses, that include heart disease and cancers in many of those vaccinated.
The Cleveland clinical study is significant given that it included 53,402 employees, of which 43,857 (82.1%) had received the influenza vaccine. The study did not include any of the common adverse side reactions, i.e. soreness, redness, or swelling at the injection site, mild fevers, headaches, muscle aches, as well as faintness and fatigue.
It would also be useful to know how much money the pharmaceutical industry makes from selling these vaccines, and the fact that the regulatory agencies recommending them are largely funded by the pharmaceutical industry. Something that should make us all pause for thought.
As shown in Part 2, like the Covid vaccines, the more shots a person receives, the more vulnerable they become to repeatedly getting Covid, not mention the harmful and often ongoing life changing side effects.
In other words if you want to increase your chances of getting the flu, or Covid, together with the related, potentially serious side effects, that include brain damage and death, then just keep getting as many as these “safe and effective” shots as you can.
Ref: https://www.medrxiv.org/content/10.1101/2025.01.30.2 5321421v3

If the current approach to health care is claimed to be the best that science can offer, then why are people in developed nations so seriously unhealthy? Nations like America whose populations receive almost 100% of the recommended regular vaccinations, and where approximately 66% of all adults take prescription drugs regularly to suppress ongoing symptoms for chronic illnesses? A pattern similarly mirrored in the UK, and where its politicians are also in bed with Big Pharma.
President Trump: ”For too long, Americans have been crushed by the industrial food complex and drug companies who have engaged in deception, misinformation, and disinformation when it comes to Public Health. The Safety and Health of all Americans is the most important role of any Administration, and HHS (Dept Health and Human Services) will play a big role in helping ensure that everybody will be protected from harmful chemicals, pollutants, pesticides, pharmaceutical products, and food additives that have contributed to the overwhelming health crisis in this Country. Mr. Kennedy will restore these Agencies to the traditions of Gold Standard Scientific Research, and beacons of transparency, to end the chronic disease epidemic, and to Make America Great and Healthy Again!”
Taken from a statement on Truth Social, and why he has appointed Robert F Kennedy Jr to oversee the Department of Health and Human Services. Nephew of U.S. president John F. Kennedy and Senator Ted Kennedy, Robert F Kennedy Jr is also known by his initials RFK Jr., politician, environmental lawyer, author and anti-vaccine activist, RFK Jr was born January 17, 1954, and began his career as an assistant district attorney in New York City. The following quotes are taken from a recent speech given to the Senate Confirmation Hearing in January 2025:
“Why are health care costs so high in the first place? The obvious answer is chronic disease.The CDC says that 90% of healthcare spending goes toward managing chronic disease, and hits lower income Americans the hardest. The President's pledge is not to make some Americans healthy again, but to make all Americans healthy again…..We will bring together all stakeholders in pursuit of this unifying goal. My journey into the issue of health began with my career as an environmental attorney working with hunters and fishermen and mothers in the small town in the Hudson Valley and along the Hudson River. I learned very early on that human health and environmental injuries are intertwined, for example the same chemicals that kill fish also make people sick. Today American’s overall health is in a grievous condition with over 70% of adults and a third of children overweight or obese. Diabetes is 10 times more prevalent than it was during the 1960s, and cancer among young people is rising. Autoimmune diseases, neuro-developmental disorders, alzheimer’s, asthma, ADHD, depression, addictions and a host of other physical and mental health conditions, some of which are exponentially on the rise.
The United States has the worse health of any other developed Nation, yet we spend more on healthcare, at least double, and in some cases triple as other countries. Last year we spent $4.8 trillion, not counting the indirect costs of missed work. That's almost a a fifth of GDP, and equivalent to a 20% tax on the entire economy. No wonder America has trouble competing with countries that pay a third of what we do for health, and have better outcomes and a healthier workforce. I don't want to make this too much about money, (because) it’s the human tragedy that moves us to care. President Trump has promised to restore America's global strength and to restore the American dream, but he understands that we can't be a strong nation when our people are so sick. A healthy person has a thousand dreams, (but) a sick person has only one. Today over half of our countrymen and women are chronically ill. When I met with President Trump last summer I discovered that he is more than just concerned for this tragic situation, and genuinely cares. President Trump is committed to restoring the American dream and seventy seven million Americans delivered a mandate to him to do just that. I promised President Trump that I will do everything in my power to put the health of Americans back on track.

Before I conclude I want to make clear that in spite of news reports, I'm not anti-vaccine (but) I am Pro safety vaccine. {Applause} I have worked for years to raise awareness about the mercury and (related) toxic chemicals. I’ve written many books on vaccines, and wrote my first book in 2014. In my advocacy I've often disturbed the status quo by asking uncomfortable questions, well I’m not going to apologise for that. We have massive health problems in this country that we must face honestly, and the first thing I've done every morning for the past 20 years is to get on my knees and pray to God that he would put me in a position to end the chronic disease epidemic, and to help America’s children. That's why I'm so grateful to President Trump for the opportunity to sit before you today….” END


The latest data from the United States is showing that like the UK, that by the time a child reaches 8 years old, a significant proportion have brain damage ranging from mild to severe learning and intellectual disabilities. A fact that should be causing a major international scandal.
"The autism epidemic is running rampant," said U.S. Health and Human Services (HHS) Secretary Robert F. Kennedy, Jr. "One in 31 American children born in 2014 are disabled by autism. That's up significantly from two years earlier and nearly five times higher than when the CDC first started running autism surveys in children born in 1992. Prevalence for boys is an astounding 1 in 20 and in California it's 1 in 12.5.”…"The autism epidemic has now reached a scale unprecedented in human history because it affects the young,” "The risks and costs of this crisis are a thousand times more threatening to our country than COVID-19”. …”Autism is preventable and it is unforgivable that we have not yet identified the underlying causes.”
"President Trump has tasked me with identifying the root causes of the childhood chronic disease epidemic - including autism," Secretary Kennedy continued. "We are assembling teams of world-class scientists to focus research on the origins of the epidemic, and we expect to begin to have answers by September."
The new ADDM report was conducted in 2022 across 16 sites in the U.S. and surveyed children aged 8 years born in 2014. This latest autism prevalence is 4.8 times higher than in the first ADD survey 22 years ago, when prevalence was 1 in 150 children. The increase in autism spectrum disorder (ASD) prevalence cannot be solely attributed to the expansion of diagnoses to include higher functioning children. On the contrary, the percentage of ASD cases with higher IQs (> 85) has decreased steadily over the last six ADDM reports to 36.1% in the 2022 survey. Nearly two thirds of children with ASD in the latest survey had either severe or borderline intellectual disability (ID).
Minority children were more severely affected. Black, Asian, and Hispanic children in the 2022 survey had higher overall ASD prevalence (3.66%, 3.82%, and 3.30%, respectively) than White children (2.77%), and were also more likely to have a more severe form of autism. Among Black, Asian, and Hispanic children, 78.9%, 66.5%, and 63.9%, respectively, had either severe or borderline ID, compared to 55.6% of Whites.This report exposes a series of critical public health crises.
For full report PDF. ‘Prevalence of Autism Spectrum Disorders - Autism and Developmental Disabilities Monitoring Network, Six Sites, United States, 2000’: https://www.cdc.gov/mmwr/preview/mmwrhtml/ss5601a1.htm
Back in the 60’s (Prior to childhood mass vaccination policies) autism very very rare at 1 in 10,000 child, but has progressively, increased. By 2023 it had gone up to 1 child in 31 and rising. In other words, like brain damage related dementia in the elderly, we are witnessing a simultaneous brain damage epidemic in children. Ranging from poor confidence, mental health issues, speech problems and learning difficulties to autism.
Could there might be a genetic predisposition? But genetic changes of such a sever nature could not occur so quickly, so we can rule that out. Even if there were genetic predisposition in some, this could not cause such a rapid escalation in brain damage in both age groups. A fact that have become an ongoing tragedy for millions of families around the world. Levels of widespread brain damage in those vulnerable of a severity hitherto unknown, and why the continual increasing of vaccines given to both age groups since the 60’s onwards, together with the evidence (See Part 5) is why immediate action is needed.
This are not normal age-related brain damage, Part 5 particularly points to brain cell death caused by heavy metal poisoning, administered by doctors, and who without doing any serious research are happy to receive the perks, while turning a blind eye to any possible risks. In other words, I believe these a iatrogenic illness, i.e. brain damage caused by medical doctors pushing unproven vaccines on the general public thus giving more billions to Bill Gates and other highly dubious pharmaceutical manufacturers.

It is an established fact that heavy metal toxicity from vaccines can, and does cause reactive brain inflammation in those vulnerable; also known as encephalitis. This would include inflammation of the hippocampus, a part of the brain crucial for memory, mental, behavioural and cognitive functions, impairment of which can lead to memory lapses, difficulty concentrating, confusion and loss of appetite, together with behavioural changes that can include aggression, impulsivity, lethargy, reduced social interaction, depression, anxiety, irritability, difficulty controlling emotions, and even psychosis. Given that mental health issues in children and adults, together with special needs with autism and dementia were relatively non existent before the introduction of neurotoxic heavy metal laden mass vaccination from the 1960s onward, are we missing something here?
Parts 4 & 5 discusses vaccine related brain damage in children and the elderly, and how both suffer similar reactive brain cavity expansion cause by brain inflammation; not to mention a similarity in some symptoms. Could this be perhaps because both are more vulnerable, i.e. infants and children that do not have fully developed brains and immune systems; on the other hand, the elderly who have naturally degenerating brain cells, and often weakened immunity, thus making both groups more vulnerable to heavy metal toxic insult and brain inflammation.

“Over the last 24 months, there has been growing evidence of a correlation between mRNA COVID-19 vaccine boosters and increased prevalence of COVID-19 infection and other pathologies. Recent works have added possible causation to correlation. mRNA vaccine boosters may impair immune system response in immune compromised individuals. Multiple doses of the mRNA COVID-19 vaccines may result in much higher levels of IgG 4 antibodies, or also impaired activation of CD4 + and CD8 + T cells. The opportunity for mRNA vaccine boosters to impair the immune system response needs careful consideration.”
In other words the Covid vaccines are causing widespread “Immunosuppression” in the most vulnerable. This explains why so many have, and still are dying as a result of weakened immunity and cancers. Therefore take note of the following official warning that speaks volumes:
“Do not administer M-M-R II vaccine to individuals who are immunodeficient or immunosuppressed due to disease or medical therapy Measles inclusion body encephalitis 4 (MIBE). Pneumonitis and death as a direct consequence of disseminated measles vaccine Virus infection have been reported in Immunocompromised individuals inadvertently vaccinated with measles-containing vaccine. In this Population, disseminated mumps and rubella vaccine virus infection have also been reported.”
The Family of a man who rapidly deteriorated and died shortly after receiving mandated Covid shots had their suspicions confirmed after insisting their father be given post-mortem examination, so as to accurately determine the actual cause and manner of his death. What needs to be understood is that when referring to “Necrotizing Encephalitis” the study is describing brain cell death, related to reactive brain swelling, and heart failure and both being caused by ongoing spike protein production caused by the vaccine.



Shortly after this data was released VAERS stopped publishing this vital information despite the fact that these reports ran into dozens of pages. Below are a small sample, published before they decided to keep this disturbing truth hidden. This means therefore, one can only assume this so called ‘adverse event’ is still ongoing.
1255336 Significant mental impacts: Depression (to the point of suicidal thoughts): Neuropathy in Face, Arms, Legs; Sensation of coldness in bones; Extreme sudden fatigue; Significant mental impacts: Depression (to the point of suicidal thoughts); Inability to concentrate; Light sensitivity; low grade headache in centre of brain; This is a spontaneous report from a non-contactable consumer (patient). A 52-year-old male patient received BNT162B2 (PFIZER-BIONTECH COVID-19 VACCINE, solution for injection, administered in left arm on 03Apr2021 10:30 (Batch/Lot Number: ER8732) as single dose for COVID-19 immunisation, in the hospital. No follow-up attempts are possible. No further information is expected.
1279726 Patient experienced fatigue, extreme body aches, fever and very extreme depression and thoughts of suicide. Refused treatment. Symptom of fever passed within 12 hours. Symptoms of severe body aches lasted 48 hours. Symptoms of extreme depression and suicidal thoughts lasted 24 hours.
1280218 1st and 2nd day after vaccine: Low fever, excruciating body pain, site injection itch, suicidal and violent thoughts, head and brain ache, dehydration, persistent migraine, injection site inflammation, and itchiness. 3rd day: Pressure pain on head and eyes, slight tightness when breathing.
1274627 Extreme anxiety, agitation, and suicidal thoughts. Patient self administered 30 mg diazepam 1 hour after onset. Symptoms have not yet resolved. Patient is currently under outpatient psychiatric care.
958443 Death by suicide: 12/26/20, self inflicted gun shot wound; found deceased by family member: DIED 12/26/2020
987946 Evening of the shot, noticed a sore arm and extreme fatigue. Following day, tired with brain fog. Third day, brain fog worsens, depression begins. Fourth day, confusion, withdrawal from interacting with others, worsening depression. Subsequent days, increasing confusion and severe memory problems. Becoming alarmed at inability to respond and to find words. By weekend, (5 days after shot) suicidal ideas, I stopped talking to people (I live alone, but would regularly speak to neighbours and family prior to this episode).
1280864 Suicidal thoughts, depression
1281670 Weeks of lethargy, tiredness suicidal thoughts and actions extreme depression, not willing to leave bed.
1285349 History of mild seasonal depression. Not medicated. First dose on 12/26, mild blues. Felt it was strange given how excited I had been to get the vaccine. Second shot 1/16 with mild expected fever. Within 15 hours developed severe depression and anxiety that has yet to dissipate, despite being medicated. Compulsive suicidal and obsessive thoughts, sobbing and generalised anhedonia (the lack of interest, enjoyment or pleasure) without any history of experiencing these thoughts prior.
1286235 Suicidal thoughts and a severe depressive episode that has been hard to break out of.
952704 Daughter called reporting to VAERS that her father committed suicide 1/16/2021 after the COVID 19 vaccine was administered 1/14/2021. Patient sought care twice at ER; first visit by ambulance around 5PM and Friday 1/15/2021 Medical Center: Emergency Room. 1st Discharge summary diagnosis: adverse reaction to COVID shot; 2nd Discharge summary diagnosis: adverse reaction to COVID shot, fever, and panic Disorder. Medical Center Discharge summary diagnosis: Adverse reaction to the vaccine, acute anxiety. Reportable patient symptoms at, 1st visit: fever, shaking stomach cramps, breathing issues. No fever, confusion and dementia type, patient would not stay in patient bed; patient would get up and sit down again repeatedly, agitated and anxious. Attempted to urinate in hospital bed. Patient committed suicide in home: DIED 01/16/2021
969344 Despite having mood disorders, I had achieved stability before the COVID-19 vaccine. But about 8 hours after receiving it, my mood crashed. I felt angry, agitated, irritable, and dysphoric. This continued for over 3 days. I felt much worse during the night, with symptoms ranging from rage and violent thoughts, desire for self-harm and suicidal ideas. I left a message with my psychiatrist. He responded and said that he hoped my symptoms would lessen the further away from the vaccine I got.
1285689 suicidal thoughts reported post Covid vaccination.
972170 Severe suicidal ideas. I acknowledge that I am bipolar, but my moods have been remarkably stable for the last several years. I have not been suicidal before this since 2007. I acknowledge that January tend to be difficult, but this was extreme, and it started approximately 12 hours after the vaccine was given. There are a lot of arguments to be had about correlation vs causation.
956131 Pressing on chest causing shortness of breath; extreme fatigue; stomach discomfort, nausea. headaches, no appetite, chills and diarrhoea. 2 days later false positive for Covid. Three days later for next 4 days, tested negative each time for Covid. Since vaccine 1 to 3 weeks later fatigue, no appetite, suicidal thoughts as if my endorphins were temporarily deleted, but endorphins returned 24 hours later. Due to the extreme side effects 1/22/21, I will not receive my 2nd Moderna vaccine.
979340 Body aches, Headache, Temperature of 100 degrees and shortness of breath that worsened, and suicidal thoughts.
1290637 Chest pain, started 04/29/2021, but managed with rest and OTC pain reliever, ended 05/02/2021. Panic attacks, started 04/30/2021, managed with Valium, ended 05/04/2021 suicidal thoughts were experienced with both doses. Dose 1, started 04/01/2021, ended 04/11/2021. Dose 2, started 04/30/2021, ended 05-04-21.
1292189 Patient presented to the Emergency Department on 4/13/21 with suicidal thoughts and was subsequently hospitalised. He is still currently hospitalised.
1292856 On 2/14 male patient woke up and couldn't move his left side and couldn't walk. Went to Emergency, numerous tests were run and there was nothing to substantiate. Emergency suggested to follow up with neurologist, who said it was possibly Parkinson's. Started getting better a few days before the second dose. Got the second dose on 2/25, and after the second dose everything was exacerbated, weight started dropping, started losing muscle tone, appetite, and extreme fatigue. Cognitive thinking was gone, almost like a psychosis, I was suicidal and I couldn't think straight.
1296525 So my Post Menopausal Depression came back with a vengeance after the second dose of the vaccine. After the first dose, I had the most painful period for 12 hours of my entire life. Turns out I was physically fine, but mentally very unwell. It felt different, similar to when I was 19 when I tried an antidepressant that made me feel actively suicidal. I don't know how to describe the difference in feeling, but it came out of nowhere and was very strong. I wanted to kill myself for half of April, and it wasn't for any reason whatsoever. So my best guess is that the second dose interfered with the balance my birth control gives me now, and the shock to my system made it even worse than it had been in the past. This lasted from the 4th, through my period, and after, until the 19th. I was barely able to take care of myself at all during this time. It was very difficult and debilitating. Also scary!
1298900 Got worse, I was sleep deprived for so long I Couldn't function and felt suicidal. Wanted commit suicide. Tinnitus and head tremors. This was reported by a patient family member or friend (subsequently medically confirmed).
1263157 Though my period ended on March 6th, normally, my period started again on the 26th. It was accompanied by much more intense pain and cramping, as well as intense suicidal ideas. That period ended after a very heavy bleeding of 4 days. I got the second shot just before my 37th birthday and the very next day I felt terrible. My entire body hurt in a way I have never experienced before. My feet hurt, my hips, extreme fatigue. That continued in varying severity. I started spotting again on April 19th, which continues until I started another period on April 23rd which just ended yesterday, the 26th. I am still very fatigued and have been dealing with extreme suicidal thoughts and uncontrollable crying.
1251028 Death by suicide sometime between late evening Wednesday, April 21st, 2021 and early morning April 22nd, 2021. He was found dead at about 8 am that morning.
1254024 Committed suicide and before had ringing in his ears: The cause of death was not reported. It is unknown if an autopsy was performed.
1256744 Visible swelling over lower abdominal region for 1 week that started about one day after vaccine. Pain over ovaries/uterus lasting for 1 week starting 1 day after vaccine. Experienced heavier than normal bleeding, bloating and cramping. With this there was extreme abnormal mood swings, severe depression, suicidal thoughts, anxiety, insomnia lasting severely for 3 days. I called my psychologist, and spoke to the nurse at my clinic and many others because it was too much to handle. I have never experienced this degree in my life. Since the mood swings and mood changes have mellowed but are still present today along with low back pain, cramping, bleeding and extreme exhaustion. I have been bleeding for 12 days. I usually bleed for 6-8 days.
1261488 Chills to the bone; she couldn't crawl in to bed, but slept for 18 hours; headache was worst than a migraine with vomiting and passed out. Arm swollen and red; she wished she was dead. Loss of consciousness and suicidal thoughts. The 65-year-old female patient received mRNA-1273 (Moderna COVID-19 Vaccine) for COVID-19 vaccination. No follow up possible.
1261511 Suicidal thoughts: This spontaneous case was reported by a health care professional (subsequently medically confirmed) and describes the occurrence of suicidal thoughts in a patient who received mRNA-1273 (Moderna COVID-19 Vaccine) for COVID-19 vaccination.

On April 10th 2025 the New York Times reported that Republican senator Ron Johnson accused the CDC of mishandling and possibly deleting key records relating to monitoring reports of adverse COVID-19 vaccine reactions.
In response to a subpoena from Sen. Ron Johnson demanding for vaccine safety data, officials at the Department of Health and Human Services (HHS) could not find the relevant records belonging to Dr. Tom Shimabukuro, the director of the CDC’s Immunisation Safety Office. “HHS officials recently informed me that Dr. Shimabukuro’s records remain lost and, potentially, removed from HHS’s email system altogether,” Johnson wrote a letter on Wednesday to Attorney General Pam Bondi, FBI Director Kash Patel and acting HHS watchdog Juliet Hodgkins.
Last November, Johnson had asked HHS, the CDC and the Food and Drug Administration to “preserve all records referring or relating to the development, safety, and efficacy of the COVID-19 vaccines.”….“Any attempt to obstruct or interfere with my investigatory efforts would be grounds for contempt of Congress,” Johnson wrote Wednesday. Under the Federal Records Act, government officials are required to preserve materials “made or received by a Federal agency under Federal law or in connection with the transaction of public business.”
In November 2023, Johnson discovered evidence that Dr David Morens, senior advisor to the Director, National Institute of Allergy and Infectious Diseases, National Institutes of Health, had instructed colleagues to comply in 2021 via Gmail. Morens later claimed he couldn’t remember whether he had deleted emails.
Johnson is now calling upon the FBI, DOJ and HHS Inspector General’s Office to probe whether Shimabukuro and other federal health officials have “deleted or destroyed official agency records.”….”I had always suspected that Dr. Morens was not the sole evader of federal record keeping requirements at HHS,” Johnson remarked.
“The extent to which HHS officials systemically mishandled, deleted, or destroyed their communications, data, and other information relating to the COVID-19 pandemic and the vaccines must be thoroughly investigated.” Contempt of Congress is punishable by up to a six-figure fine and 12 months in prison.

To quote the Daily Mail: Referring to US Health Secretary Robert Kennedy, President Trump stated, “There's something very wrong, so, we’re going to find out what it is, and there is nobody better than Bobby (R F Kennedy) and all the people working with you.” The CDC will study the potential link between vaccines and autism, sources have revealed. It is unclear whether newly appointed health secretary Robert F Kennedy Jr, who has long been skeptical of vaccines, is involved in the planned study or how it would be carried out. Kennedy, whose role includes authority over the CDC, has long sown doubt over the safety of the measles, mumps and rubella (MMR) vaccine, along with Covid shots made by Pfizer and Moderna.
To make matters worse, the latest Yale University research confirms what many researchers warned at the beginning, i.e. that production of the spike protein can persist in your body for years, thus continually draining the body’s immune strength, causing ongoing symptoms that include chronic illnesses, lethargy and brain fog. The research led them to believe that these people were suffering from Post-Vaccination Syndrome due to the levels of spike protein still circulating in their blood; presumably a condition previously claimed to be long COVID. In other cases, other viruses that were dormant in their bodies, such as Epstein-Barr, were reactivated.
‘medRxiv’ Yale’s preprint server, also reported related immune system exhaustion and other biological changes following vaccination, and why, next they want to determine how widespread PVS actually is, and who is most at risk. Immunologist and computational biologist Jessica Rose, Ph.D. said she wasn’t surprised by the study’s findings, “Since the coding material for the spike protein … is introduced to the human body via lipid nanoparticles, it can literally be tracked to anywhere in the body via the bloodstream.”
Furthermore, member of the World Council for Health steering committee, Christof Plothe, D.O. has stated concerning the COVID-19 mRNA vaccines:
“Vaccines that essentially are turned into mini-factories, instructing our own bodies to produce one of the most pathogenic proteins known to science, and we still don’t know how long this production might continue. There’s a high probability that the genetic instructions could have integrated into the human genome, potentially making its effects of this gene therapy life-long.” In other words, the vaccine has changed human DNA to the extent that our DNA is programming the immune system to continually attack its own body, thus resulting in numerous chronic diseases and related premature death due to weakened immunity, as all the evidence shows.
When the UK Health Secretary was recently asked during a Radio 4 interview why the annual cost of health-related benefits, due to a continued increase people to ill to work, has risen from 50 billion pounds to over 100 billion pounds in the last few years, he ignored the elephant in the room, i.e. parallel worldwide elevated rise in strokes, heart conditions and death rates that have continued since the rollout, he replied, “we have no idea.” Not to mention the significant increase in youth mental health issues, and the fact that between 2012 and 2022 there has been an almost 70% increase in the number of children and young people being admitted to general acute medical wards in hospitals in England.
According to NHS England and citing The Mental Health of Children and Young People in England 2023 report, it found that 20.3% of eight to 16-year-olds had a probable mental disorder in 2023. Among 17 to 19-year-olds, the proportion was 23.3%, while in 20 to 25-year-olds it was 21.7%. All representing rising rates of probable mental disorders between 2017 and 2020, and continuing at similar levels in all age groups between 2022 and 2023.
In Part 5 we discuss studies showing how the healthier unvaccinated children have no ADHD, and also suffer far less vaccine-related autoimmune illnesses, so prevalent among vaccinated children, i.e. allergies, learning difficulties and asthma etc. Part 5 also discusses how exposure to heavy metals not only kills brain cells, they are poisons that can negatively impact mental health, leading to similar conditions in more susceptible brains, such as the young and elderly. Symptoms such as loss of coordination, bladder issues, memory loss and related cognitive dysfunction, together with learning difficulties, behavioural changes, anxiety, and depression etc.
NB US Health Secretary Robert F Kennedy Jr is also the founder, and former chairman and chief litigation counsel, for ‘Children’s Health Defense; https://childrenshealthdefense.org/ A nonprofit activist group that has filed nearly 30 Federal and State lawsuits since 2020, many challenging vaccines and public health mandates.
RFK Jr’s reputation as a resolute defender of the environment stems from a litany of successful legal actions. He was named one of Time Magazine's “Heroes for the Planet” for his success helping the Riverkeeper project lead the fight to restore the Hudson River.
Autism, like dementia can be a condition of slow progression, and like dementia, the severity of both diseases varies from patient to patient, but usually the ability to communicate with others is always affected. Note also the related dementia mortality rate is now the major cause of death in the elderly, increasing by almost 150% in the past 20 years, i.e, 1 in 3 adults will die from Alzheimer's or another form of dementia. The question therefore is why are brain diseases among the more vulnerable, ie developing and aging brains, reaching epidemic proportions? With regard to autism, a secret CDC Meeting held in 2017, at Simpsonwood was convened to compare the health outcomes of babies and children who had received vaccinations from the day of birth, as well as children who had received vaccination after 60 days of life, in contrast to children that did not receive any vaccinations.
What they found, but decided to keep secret so as to cover up the vaccine related mercury dangers to brain development, was that the children who had received vaccination had a staggering 1135% greater chance of being diagnosed with autism, when compared to those that did not receive vaccinations.
There are studies also consistently showing that boys are much more likely to be diagnosed with autism than girls, and that poor and black children are at a higher risk.
But the trend, like dementia among the elderly, continues unabated. For example, since 2017 autism among American children and teens, like the UK, has surged by a further 50%. See Part 6: Vaccine Heavy Metal Brain Damage & Studies Showing the Unvaccinated are far Healthier. Ref: https://childrenshealthdefense.org/ to download: The-Simpsonwood-Documents.pdf
The much maligned Dr Andrew Wakefield is among the most controversial figures in autism circles. His research regarding whether the Mumps-Measles-Rubella (MMR) vaccine has caused the escalation and ongoing epidemic of brain damage labelled autism has created a huge rift.
Dr. Wakefield is an academic gastroenterologist (digestive system specialist) and surgeon with a special interest in inflammatory diseases. Born in Britain in 1957, he was educated in Canada and became a physician at the Royal Free Hospital in London. Early in his career, Wakefield made an important contribution to medical research when he identified the cause of Crohn's disease, a major gastrointestinal illness, as decreased blood flow to the intestines. Soon after this discovery, Wakefield began digging into the question of whether it was measles virus from the MMR vaccine that caused the blockage of blood flow leading to Crohn's.
In 1995, Dr. Wakefield was approached by a group of parents who told him that their children had become autistic following the MMR vaccine. They asked him to look into a possible connection, after parents saying, “my child was perfectly fine until they received the MMR vaccine and that they either had seizures, or slept for three days and never woke up, or that the light had gone from their eyes, in addition to loss of speech and social interaction etc, Dr Wakefield subsequently agreed to do so.
In fact he was one of the first to make the connection between post vaccine reactive bowel inflammation and what has since become an epidemic of "leaky gut syndrome, or “increased gut permeability.” A leaky gut has also been widely linked to many of the following possible symptoms: chronic diarrhoea, constipation or bloating, nutritional deficiencies, fatigue, headaches, confusion, difficulty concentrating, skin problems, such as acne, rashes, eczema, joint pain and widespread inflammation. In addition to leaky gut the related long-term intestinal inflammation has also been linked to an increased risk of colon cancer, as well as gut perforation or bowel obstruction, that can lead to numerous medical emergencies.

In 1998, Wakefield and a group of colleagues published a research study which linked inflammatory bowel symptoms in autistic children to the MMR vaccine. That study, published in the respected British medical journal The Lancet, launched a massive anti-vaccine movement in the United Kingdom, the United States, and around the world.
In addition to being castigated and slandered Dr Wakefield's influential research paper was retracted by the British medical journal The Lancet in 2010. But in spite of medical ‘professionals’ and the highly profitable vaccine industry’s efforts, his work remains a potent force in the autism community.
In his book ‘How to End the Autism Epidemic’ author J.B. Handley presents an intellectual, fact-based argument on how vaccines trigger autism, drawing on scientific evidence that has emerged in the past five years from researchers outside the United States. In it he confronts and dismantles the most common rhetoric from the CDC, i.e that all vaccines are safe and effective.
If the science is settled, i.e. that vaccines do not cause brain damage, then why is the rate of autism still increasing? In the 1960s, the CDC vaccine schedule called for 5 total vaccines, today it is a staggering 72 toxic laden injections. If the science is settled, then why has The Department of Health and Human Services Vaccine Compensation Program actually acknowledged that vaccines do in fact cause autism? See also vaccine induced brain damage and comparative health of both vaccinated and unvaccinated children in Part 5.
As you may have noticed, like the Covid rollout, scare tactics are Big Pharma’s weapon of choice when it comes to getting the public back on board with vaccines, such as the much publicised recent outbreaks of measles, which as is claimed America, the spread is being fuelled by low vaccination rates, and especially among young children, caused, they believe, by fear due to vaccine damage mis-information. In 2019. The Washington Post even warned that, “Unvaccinated children banned from public spaces amid measles outbreak in New York Suburb.”
Thanks to a case brought by an anti-vaccine group, on August 29, 2023, attorney Aaron Siri presented evidence sufficient to cause a judge in a Mississippi lawsuit to overturn a previously-issued vaccine mandate, and by using the CDC’s own statistics. Including a 1900 to 1960 chart showing the recorded death rates for measles, per 100,000 per population, bearing in mind the measles vaccination programmes did not begin until 1963.
Before anyone was being vaccinated against measles there had already been a precipitous decline in measles thanks to improved sanitation and nutrition etc. But when one considers that even at the highest levels, at its worst, measles was only killing 13 in 100.000 and by 1960, before the introduction of blanket vaccines, measles deaths were virtually non existent. Before the mass vaccine rollouts it used to be that everyone who contracted measles gained natural lifetime immunity by the age of 15.
This is because measles is a known self-limiting childhood infection and most cases are benign and not even reported, so why the need for harmful vaccines that are neither safe or effective, and that by and large don’t work? Through the Freedom of Information Act documents have been obtained, used to licence these vaccines back in 1978 based on clinical trials that used a total of only 834, split into separate groups to minimise the numbers, i.e one group of a couple of hundred plus for measles, the same for mumps and rubella, made worse by very scant follow-up procedures.

For example, “Each child will be followed clinically for 42 days following vaccination.” Far shorter that standard drug trials, some as long as six years. In other words, any adverse health consequences were no longer considered causal after day 43. But as many people have discovered since the Covid shots, many serious symptoms, some life threatening can occur months and even years after getting vaccinated. All vaccines cause some degree of autoimmune reactions which explains why autoimmune diseases are so common today, i.e. the 10 most common being: Inflammatory bowel disease (Crohn's disease, ulcerative colitis) rheumatoid arthritis (RA), lupus, type 1 diabetes, multiple sclerosis (MS), scleroderma, psoriasis and psoriatic arthritis; none of which will usually become evident within 42 days. The vaccine manufacturers have to by law list all related known adverse reactions, many of which turn out to be life changing. For example one of the known reactions is encephalitis, aka brain swelling and is directly linked to autism and dementia as shown in part 5.
Bearing in mind that no study has ever been carried out to examine these well known reactions in children, or why some children, i.e. particularly black children are more susceptible. Why is it that in spite of these facts the design and reporting of safety outcomes in MMR vaccine studies, both pre and post-marketing, are totally inadequate.
This remains the case in spite of the CDC acknowledging that “severe problems have been reported after a child gets MMR vaccine that include: deafness, long-term seizures, coma, lowered consciousness and permanent brain damage.
The following adverse reactions include those identified during clinical trials or reported during post-approval use of MMR vaccine or its individual components: encephalitis, encephalopathy, (brain swelling) Guillain-Barré Syndrome, acute disseminated encephalomyelitis, transverse myelitis, febrile convulsions or seizures, ataxia, polyneuritis, fever, headache, dizziness, malaise, irritability, vasculitis, pancreatitis, diarrhea, vomiting, parotitis, nausea, thrombocytopenia, purpura, leukocytosis, anaphylaxis, anaphylactoid reactions, swelling (peripheral and/or facial), bronchial spasm, arthritis, arthralgia, myalgia, polyneuropathy, ocular palsies, peripheral nerve abnormalities, pneumonia, pneumonitis, sore throat, cough, rhinitis. measles-like rash, ear nerve deafness and otitis media, optic neuritis, conjunctivitis and urogenital problems.
One of the largest outbreaks of measles in recent decades was labelled the ‘Disneyland Outbreak’ in California between 2014 and 2015 and was used to push the SB277 measles vaccine. In June 2015, California passed a law called SB277 that took away parents' rights to exempt their children from mandated vaccines for religious and personal reasons, leaving only a narrow, hard to get medical exemption option.
The claim at the time was that by removing any exemptions this would prevent any further outbreaks, given that all children would be vaccinated. Just like the Covid scam, the government spread the unfounded lie that it was the unvaccinated who were to blame for spreading Covid; we now know the exact opposite to be true as clearly shown in Part Two. Like the Covid lie, according to their own data, subsequently released from the Department of Public Health shows the reasons used to take away any parental right to exempt their children was also based on lies. For example, the distribution and hospitalisation status of the California Measles outbreak cases show the majority were adults.
The data gets even more suspicious when one considers that 62% of all recorded cases were ‘immunisation status verified’. Furthermore, given the fact, that like the rest of us, the vast majority had also been measles vaccinated at some point, suggests a total vaccine failure to protect both adults and children. To add insult to injury when the California Department of Public Health looked at the specific strains they found a significant proportion of those who became ill had been contaminated by the ’31 genotype A strain’, i.e. the strain used in the vaccines, thus showing it was the vaccines that had caused many to fall prey to measles, as is the case with Polio vaccines, see Part? Ref: https://thehighwire.com/

Like many other countries, each year American babies (1 year old and younger) receive more than 10 million vaccinations, after which these babies are known to suffer from serious, reactive life-threatening illnesses and medical events, such as Sudden Infant Death Syndrome, but reactive fevers are by far the most commonly reported adverse event. For example a study published in the National Library of Medicine concluded that the proportion of vaccination records requiring antipyretic drugs (medications that reduce or relieve fever by lowering an elevated body temperature) was over 77%.
It is a well documented fact that infantile exposure to heavy metals such as aluminium and mercury i.e. thimerosal, an active ingredient in many vaccines, are not only linked to reactive brain fever but also the development of neuro-developmental disorders such as ADHD, autism and speech delay.
In 1962, children received just five vaccine doses. As of 2023, children up to age 18 receive 73 doses of 16 different vaccines; the cumulative effects of this childhood vaccine schedule have never been tested. In addition to neuro-developmental disorders research also shows that vaccinated children experienced significantly higher instances of various health issues, including allergies, asthma, behavioural issues and gastroenteritis. The 1986 National Childhood Vaccine Injury Act requires the U.S. Department of Health and Human Services to report on vaccine safety every two years, but to this day the agency has never submitted a vaccine safety report to Congress. In other words, the Health agencies have data on the health outcomes for vaccinated and unvaccinated children, but are refusing to make it public. There are multiple mechanisms of potential harm when it comes to vaccination, one of them also involves aluminum, the most commonly used vaccine adjuvant.
There are numerous studies confirming the links between vaccinated children and neuro-developmental disorders. (NDDs). For example the graph below is taken from a PEER REVIEWED, study of children enrolled in the Florida Medicaid program between 1999 and 2011 and concluded that:
1. Vaccinated children were significantly more likely than unvaccinated children to be diagnosed with the following NDDs: ASD (autism spectrum disorder is a developmental disability that affects how a child interacts, communicates, and behaves, often appearing in early childhood) hyperkinetic syndrome of childhood, epilepsy or seizures, encephalopathy, tic disorders, and learning disorders. 2. Increasing numbers of healthcare visits that included one or more vaccinations were associated with higher risks of diagnosis for ASD, suggesting a dose-response relationship. 3. Preterm birth and vaccination increased the odds of being diagnosed with all measured NDDs beyond the effects noted for only preterm birth and vaccination alone. 4. Children born preterm and unvaccinated were no more likely than children born at term and unvaccinated to be diagnosed with ASD, hyperkinetic syndrome, encephalopathy, tic disorders, and learning disorders. They did, however, have higher odds of seizures/epilepsy. The results of this study add to a growing body of evidence suggesting that vaccination may be associated with significantly increased odds of various medical conditions, including NDDs. Ref: https://publichealthpolicyjournal.com/ethics-in-science-and-technology/

All of which are discussed further in Parts 3 and 5, but the thing to note from the above study is the reactive encephalopathy, a general term for brain dysfunction, caused by reactive autoimmune brain swelling and fevers.
This is important because a review of studies published in 2025 in the journal Environmental Health concluded there is an association between commonly used painkillers given to infants and children to alleviate vaccinated related fevers that actually contribute to the development of ADHD and Autism. In the UK and America doctors and health officials recommend using drugs such as paracetamol (calpol) and/or acetaminophen (Tylenol), ibuprofen Advil, Motrin, and others to lower temperature and other related symptoms.
President Trump also recently cited data showing a rapid increase in autism diagnoses in recent years: “Since 2000, autism rates have surged by much more than 400%,” he said. “Instead of attacking those who ask questions, everyone should be grateful for those who are trying to get the answers to this complex situation.”
John Gilmore, executive director of the Autism Action Network, said today’s announcement is significant because it “has shattered two of the cardinal taboos about autism causation.” He said: “First, that [autism] has an environmental cause. Official science has looked almost exclusively for genetic causes for autism, even though no single gene or combination of genes has ever been shown to be statistically significant, but that’s all we have done for more than 20 years. And when there is an environmental cause, somebody is responsible for putting that thing in the environment. “Second, pregnant women were taking Tylenol on the advice of their physicians, and probably ignoring the advice of their grandmothers. That means this is an iatrogenic (doctor induced) cause of autism, and it is highly unlikely to be the only one.”
Although most consumers believe that over-the-counter medications are safe and effective, recent data offers more evidence that acetaminophen during pregnancy increases your child’s risk of attention-deficit/hyperactivity disorder. In fact there is a great deal of data that documents disturbing links between acetaminophen use during pregnancy and neurological problems in children, including poor gross motor development, communication issues, increased risk of pre-eclampsia and a moderately increased risk of undescended testicles in boys.
Acetaminophen is the most common drug ingredient on the market and the FDA has known about autism risk for years, as newly surfaced emails obtained by the Daily Caller News Foundation confirm. They show that as long ago as 2008, officials at Johnson & Johnson, the original maker of Tylenol, were privately concerned about what they believed to be credible evidence of a possible link between autism and acetaminophen. Makers of Tylenol and the U.S. Food and Drug Administration (FDA) knew for years about the likely association between the drugs also used during pregnancy and the onset of neuro-developmental disorders, including autism, according to documents obtained in lawsuits against Kenvue. “The weight of evidence is starting to feel heavy to me,” said Rachel Weinstein, U.S. director of epidemiology for Johnson & Johnson’s pharmaceutical division, Janssen, in an email commenting on several studies showing the link. Emails were also found indicating that J&J considered funding studies on Tylenol’s possible link to autism, but decided against “sticking their necks out,” worried their studies could confirm the findings.
As early as 2019, FDA study authors recommended that the labels be revised to advise pregnant women to “be careful about casual use of acetaminophen when it is not strongly needed for pain or other purposes.” In other words using acetaminophen based drugs found in over 600 medications that are commonly consumed during pregnancy can also increase your child’s risk of autism spectrum disorder. The FDA also grew concerned with the mounting evidence of a link between acetaminophen and neuro-developmental disorders, beginning with a publication in JAMA Pediatrics in 2014 and followed by several major publications over the next several years, according to psychiatrist David Healy. Another study published in 2020 in JAMA Psychiatry strengthened the link between acetaminophen use during pregnancy and ADHD and the risk of ASD.
For further information see: Mawson_Jacob_SciencePublicHealthPolicyAndTheLaw_v6.2019-2025.Jan_2025.pdf

In addition to Bill Gates Demanding the right to censor all the “Insane People” who oppose him on the Internet as the world continues to wake up to the crimes of the globalist elite and the public mood worsens, the elite are now floating the idea of a “Covid amnesty” for all the elite decision makers who ruined millions of lives by enforcing draconian lockdowns, masks on children, and barbaric vaccine mandates. Not to mention the continued increase in deaths, blood clots, strokes, turbo cancers and life changing neurological complications.
According to a recent ‘Atlantic’ article, the elite, including Dr. Anthony Fauci, Bill Gates and Joe Biden to name a few, should be given a free pass and granted amnesty against prosecution as more and more evidence of their malpractice and outright criminality continues to surface. It sounds like the elite are aware the dam wall is about to burst and their plannned-demic crimes are about to be exposed to the mainstream. And the elite are rightly terrified of the masses rising up, waking up and rising up against them.
Given all that we have been through in recent years, are we really just expected to grant a pardon to the elite who, over and over, proved themselves to be incompetent at best, and in many cases, outright tyrants? Absolutely not. Are we expected to erase the record of those responsible for leaving sick children to waste away in hospitals all alone, for separating husband from wife, for stopping families from holding the hands of the dying or gathering for their funerals? No, no, and again, no.
After mandates forced people out of jobs, destroying livelihoods and lives, and the vaccine-turned-therapeutic was exposed as failing to stop transmission, are we really expected to stop asking about its potential side effects, or the relationship between Big Pharma companies and the FDA? Are we really to let bygones be bygones for masking and lockdowns that will set students back for a decade, that shuttered businesses across the country, that multiplied deaths of despair? The other people are “the experts” and, more importantly, “the authorities.” And when they are wrong they must admit it, and be held accountable. That is what makes them, in our modern democratic and scientific society, authoritative: accountability to the public record. It was the so-called experts and public authorities who were the ones making (wrongly) all the assessments, predictions, and decisions on behalf of ordinary people, and they are supposed to be judged by the accuracy and utility of those assessments, predictions, and decisions.
The reckoning has not yet begun. The people who got it right, for whatever reason, may want to gloat. Those who got it wrong, for whatever reason, may feel defensive and retrench into a position that doesn’t accord with the facts. Throw them all out. “Getting something wrong” might not always be a moral failing, but it is a professional failing, in an expert or public official. They failed at their job. They should not be allowed to keep it.
Furthermore by any standards, these are crimes against humanity and for justice to done criminal proceedings for all involved is the only way to ensure this is not repeated. Because make no mistake, they already have the next plannned-demic ready and waiting. So no pandemic amnesty, but instead capital punishment for all those who knew what they were doing, and will again, but only if we let them. NB: The above are extracts are originally from ‘The Atlantis’ news, and from ‘News Punch.’ It can also be found on‘The People's Voice’ website: Ref: file:///Users/luisalicea/Desktop/The People's Voice - Where Mainstream Fears to Tread.webarchive

A study by Dr Wilson Sy found over 90 per cent correlation between midazolam use and excess deaths in 2020, and that it was highly likely the UK's excess deaths were caused by the use of this drug and NOT to a virus. The report’s conclusion suggests ‘systemic involuntary euthanasia within the NHS.’ The government report included a panel of doctors and professors describing the government approach as a 'dangerous protocol.’ Not surprising given that the use Midazolam with morphine is known to suppresses respiratory systems, and so proved fatal to those already fighting off the illness. Deaths hastened thanks to NICE (National Institute for Health and Care Excellence) guideline NG163, which recommended the combined use of midazolam and morphine to treat covid.
Official government figures now confirm, that as discussed in Part 2, the alarming number of excess deaths throughout Covid, were not mainly due to a SARS-CoV-2 virus, as maintained by the media, but instead linked to deliberate government policy that included enforced excessive use of the deadly drug midazolam. Midazolam is most commonly used for sedation in intensive care units (ICUs) for severe epilepsy, and in palliative (end of life) care to manage extreme agitation or restlessness. The UK Government, Amnesty International, and the Care Quality Commission have all since acknowledged systemic dysfunctions, including widespread use of ‘Do Not Resuscitate’ instructions that also contributed to so many excess deaths.
In March 2020, then health secretary Matt Hancock ordered a huge supply of the drug from a factory in France. Around the same time, NICE guideline NG163 was introduced. The official story is that in 2020, the UK recorded approximately 705,636 total deaths, with around 74,917 attributed to covid. The number of Excess Deaths, in 2020 was an estimated at 50,000 to 60,000 above historical averages, according to the government narrative, all linked to the pandemic's impact, but Dr Sy's study tells a different story. The enforced protocol for covid, stated above, led to the huge spike in care home and hospital deaths which occurred. Families had discovered their relatives in care homes or hospitals, whilst they had been forbidden to visit them, had been given deadly cocktails of midazolam and morphine and had died as a result. These victims were not terminally ill, they weren't suffering from a virus, and many were not elderly.
Findings that incontrovertibly shifts the narrative from viral impact to ‘medical intervention.’ Not to mention the excess deaths appeared simultaneously across all English regions, and as such inconsistent with the natural spread of a contagion.

It would seem, whether you're young or old, terminally ill or not, involuntary euthanasia became accepted as a form of hastening people’s deaths without any consent and has been shown above to have been rife during the pandemic. It wasn't just the elderly and terminally ill who were the victims; many thousands have died from all kinds of questionable and sinister causes in the UK over the last five years.
Some of the stories told were hard to comprehend, especially those that focused on the apparent culling of some of the most vulnerable members of society in hospitals and care homes. Coming to light now, however, is a vast array of incontrovertible evidence in the form of medical records, drug charts and witness and expert testimony. It is proof that many innocent souls were involuntarily euthanised via certain NHS protocols and NICE (National Institute for Health and Care Excellence) guidelines.
“In May 2020, while writing an article on Do Not Resuscitate (DNR) orders (initially commissioned by The Telegraph), I spoke with a whistleblower cardiologist who told me blanket DNRs were being put on a whole new range of people with the 'pandemic' being used as the reason. Instead of DNRs being put on the terminally ill as they always had been in the past, they were now being put on anyone over the age of 60, the mentally and physically disabled, people with mental health issues of all ages - even on children with autism!”
“The doctor's actual words at the time were: "I am horrified by what is happening at NHS hospitals across the UK right now. All patients over 60 automatically get a DNR, without them or any family members being consulted.”
"I've seen the forms in their files with my own eyes. It's not just the over 60s that get them, I've seen them being put in place for young people with mental health issues, for physically disabled people of all ages and for autistic people. We had a schizophrenic woman in her early 20s admitted recently and I found a DNR form in her file. She hadn't been asked whether she wanted one or not.”
“This doctor told me that individuals who would otherwise survive were being left to die, and added that many were being actively euthanised. In 2021, while I was making the documentary A Good Death, I set up a WhatsApp support group, initially for the contributors to the film. There were about 15 of us in the group at the start; there are now 170. Among those are at least ten whose loved ones were 70 or under when their lives were cruelly snuffed out - some over a matter of hours with deadly cocktails of benzodiazepines and opioids (usually midazolam and morphine).”
Stevie Kennedy says her 57-year-old mum, Angela, was murdered in hospital after being overdosed with midazolam and oxycodone in November 2020. "My mum was hospitalised on October 3, 2020. She suffered from leg ulcers, and the pain had become so bad that she was screaming in pain and terrified she was going to have a heart attack. She couldn't stand or walk at all that day. "She was in hospital for eight weeks, treated terribly, sent to the ICU (intensive care unit), and had her right to bodily autonomy violated as they plied her with drugs. One day my brother went to visit her. She was screaming at him to pull off the bandages they had forced on her ulcers without giving her pain relief first. "He got the bandages off her, but the nurses yelled 'you're not a doctor' at him and three of them tried to physically drag him out. After nearly eight weeks there, two occupational therapists said. her progress had been amazing and said she'd be able to go home soon. The following day, my mum's asthma was bad, "I was told she had covid and that if she got any worse they would 'not escalate’.
My brother and I contacted the chief executive by email and told them our mum did not consent to a DNR and neither did we. We then got a call, telling us to come to a meeting. There were seven of them and they kept interrupting us and contradicting themselves, trying justify leaving our mum to die. "They never mentioned the midazolam they were giving her, nor did they tell us they had withdrawn her regular meds. They let us see her. She seemed more drugged than ill. She was lucid but incredibly distressed. She said 'I don't consent to a DNR' and 'I don't trust them'.
I told her to keep fighting. That night, we were called and told our mum was dying - that she was taking her last breaths. I asked if they'd taken her off the respirator; they said yes. I asked if they'd taken her off the respirator while she was still breathing and they said yes. I told them to put her back on the respirator immediately. I also reminded them that she did not consent to a DNR. "We argued with them for ten minutes before they told us she had actually already died. In the notes, there are two different times of death. It says she was dead when they found her and that she'd taken off the heart monitor and respirator herself. The drug chart shows she was overdosed with midazolam."
In her new book, Murdered By The State, Jacqui Deevoy states: “As many of you will know, I’ve been trying for the last four and a half years to highlight and expose the horrors of involuntary euthanasia within the NHS.
Innocent people are having their deaths hastened and their lives ended prematurely in UK hospitals, hospices and care homes. It’s been happening for decades but was cruelly and criminally ramped up during the faux pandemic. The only way for me to get the word out in 2020 was by writing articles, doing interviews and sharing my discoveries on social media. I was banned 11 times in 12 months that year on Facebook and was suspended on Twitter from August 2021 until January 2023.

I started speaking out about the all-too-frequent murders in hospitals, hospices and care homes in December 2020 after being interviewed by renowned author and orator David Icke. There was a huge response to that broadcast so I set up a support group for friends and relatives of the victims of involuntary euthanasia. Because the mainstream media refused to publish the story (and despite two editors of national newspapers saying it was “front page news”), I went on to produce two documentaries - ‘A Good Death?’ with @ickonic in 2021.
(https://rumble.com/v3u1rep-uncovering-the-controversy-ickonics-original-documentary-a-good-death.html) and ‘Playing God’ in 2024 (https://live.childrenshealthdefense.org/chd-tv/events/playing-god/playing-god-premier/).
Both have been seen by millions worldwide, but still the mainstream media don’t want to know. Support my work if you can. These projects take a lot of time and energy. Hearing such horrific tales and spending weeks editing each one takes its toll on my mental and physical health. I can’t do it alone. Thank you. https://www.crowdfunder.co.uk/p/murdered-by-the-state


A Dutch court has ruled that Bill Gates will face trial in the Netherlands over his involvement in misleading the public about the safety of COVID-19 vaccines. The case, brought forward by seven plaintiffs who claim to have suffered serious vaccine injuries, marks a significant blow to Gates, who has been a key figure in pushing COVID-19 vaccination efforts worldwide. The court ruled that Gates, who attempted to have the case dismissed or contest the court’s jurisdiction, was in the wrong. His legal challenge was dismissed, and as a result, he has been ordered to pay the legal fees of the plaintiffs.
Claims that also involve former Dutch Prime Minister Mark Rutte, Pfizer CEO Albert Bourla, and members of the Dutch government’s COVID-19 “Outbreak Management Team,” misled the public about vaccine safety. Like Big Pharma, Gates has managed to get away with it for so long because he is a major financier behind WHO and other Global health organisations. Gates also bankrolls mainstream media outlets thus ensuring they never report on him negatively.
The case also references Gates’ role in international initiatives like the World Economic Forum’s “Great Reset” and Gate’s involvement in global vaccination programs like the Gavi Vaccine Alliance, an international organisation that promotes widespread access to vaccines for children living in the world's poorest countries. For decades Bill Gates has committed crimes in broad daylight conducting experiments on vulnerable children in Africa and India and discussed in Part 6.
Independent journalist, Erica Krikke who has been covering the case, sees the ruling as significant, stating that even high-profile figures like Gates must answer to the court. This case could potentially set a global precedent for plaintiffs suing high profile individuals or organisations for vaccine-related injuries, especially when defendants reside outside the plaintiffs’ country. Naomi Wolf, editor of “The Pfizer Papers: Pfizer’s Crimes Against Humanity,” claims that both Pfizer and the U.S. Food and Drug Administration (FDA) were aware of the severe adverse effects of the COVID-19 vaccine early on, yet continued to promote its use.

Gates tried to argue that as a U.S. resident, the Dutch court did not have jurisdiction over him, but the court found sufficient grounds to assert jurisdiction. As a result Gates is now panicking, even begging the judge to dismiss the case, shamefully arguing that if he is held to justice in the Netherlands there will be a contagion effect. Gates is one of the key players who masterminded the planned global vaccine rollout that is now linked to millions of deaths, and part of a chilling agenda rooted in eugenics and depopulation and why understanding the bigger picture is essential, set out in Parts 2 to 7, keeping in mind that, as the saying goes, “truth can be stranger than fiction.”


Although just outed, ex-PM Orban was on the money: “This is against us and about how to change Europe; and how to get rid of Christian, conservative, national political leaders and voters, and how to make them insignificant.” He also said, “I remember Mr. George Soros published his plan in English in a Project Syndicate publication. It was done 2015, September 26. Quoting from the same document, “the EU has to accept at least a million asylum seekers annually, and that adequate financing is critical. And why he (Soros) had proposed to issue long-term Euro bonds for financing the migration crisis and the migrants social and welfare taking care when they arrive to the European Union.” And that, “safe channels must be established for asylum seekers starting with getting them from Greece and Italy to their destination countries.”… “So we are fighting again an organised gang called Empire of George Soros. And NGOs who are just supporting everybody who is transgressing our legal system and our regulation and financing illegal activity against our nation. So, this is why the story is not just about migration, but it's about how this European Union is working, and how George Soros was able to take captive the main positions inside many institutions of European Union, buying out MPs and other leaders. And in order to execute the plan which is written and it's against all the Christian and nation-based political forces. It's against us. It's about how to change Europe and how to eliminate and push aside all the Christian conservative national based political leaders and voters from the European Union decision making bodies. So, this what all this migration about, not just about migration.

The United States was in fact founded by Freemasons and is still largely run by the same secret brotherhood; a fraternity steeped in blackmail and coercion. The ongoing Epstein saga should tell you all you need to know about Trump, the British Royalty, Jimmy Saville and Freemasonry. Why are they all still free? The answer should be obvious. Criminal governments are those that have been bought and paid for, and as such pass laws that benefit their criminal paymasters. Be they bankers, big business or Big Pharma, as the evidence clearly shows in Part 2. Corrupt governments that have been deliberately steering all of us toward a New World Order and One World Government. But only after they have achieved total chaos through financial hardship and wars. Culminating in what they hope will be limited nuclear destruction, after which they intend take control, together with the help of A I frequencies discussed in part 4.
Mad? Of course, but nevertheless this is today’s reality, whether we like it or not. But we are now reaching the point where A I is about to come into play and discussed more fully in Part 4. Who can deny the existence of a world-wide network consisting of 5G towers and devices that since Covid rapidly expanded. A smart grid system deliberately designed over decades, and capable of using EM frequencies powerful enough to keep humanity in perpetual submission. Starting with 5G, then escalating to 6G and 7G, these are not only weapons-grade frequencies, they are also designed to form new A I compatible neural circuits by using synthetic biological neural pathways compatable with the injected Covid nanotechnology. In other words, A I synthetic neural circuits that are capable of mimicking human neural pathways, and why injected vaccine nanotechnology was essential to achieve this. See Part 4.
This is why the Covid vaccines contain highly EM conductive materials such as graphene, that together with the injected nanotech are designed to link the human brain and nervous system to 5G powerful external digital networks capable of wreaking havoc on people’s physical and mental health. This is not just a mere possibility, it has been deliberately engineered for this purpose, and why trillions of injected synthetic RNA packets have entered the body’s lymphatic pathways and responsible for causing blood clots, together with previously unknown fatal cardiovascular diseases in young people sometimes referred to as the ‘Sudden Death Syndrome.’
A planned madness that mirrors Huxley’s infamous novel "Brave New World," in which he envisioned a future society characterised by technological control, social conditioning, and manufactured drugged happiness. A society that prioritises stability and conformity over freedom. To be achieved through genetic engineering, psychological manipulation, that included (EM directed) sleep-learning. A world where reproduction would become obsolete, and like the film ‘The Matrix’ where all human beings are scientifically engineered to fit their societal roles.
George Orwell also foresaw the severing of bonds between families and individuals, thus eroding all trust and love, while fostering loyalty only to the state. Is this not already happening? The recent frenzy around redefining gender norms is just another psychological operation designed to normalise the absurd; but in reality keeps the masses distracted. Please watch the video at the end of this page by someone who was on the inside to get a better understanding of what the Covid Vaccine Rollout was really all about.